Often, it starts subtly. You might notice a small lump in the palm of your hand. It isn’t painful, but it's firm and a little odd. Then you start to notice you're struggling to lay your hand flat on a table, or your fingers don’t extend like they used to when you stretch. Gripping a steering wheel, shaking hands, or even putting gloves on begins to feel different. Over time, one or more of your fingers start to curl inward toward the palm. This is often how Dupuytren's Contracture begins. A subtle, creeping change that slowly starts to change your hand function and your daily routine.
What Is Dupuytren's Contracture?
Dupuytren's Contracture is a hand condition where the tissue beneath the skin of your palm thickens and tightens over time. This fibrous tissue, known as fascia, can form cords that pull one or more of your fingers into a bent position. Once a finger is bent, it may not straighten fully, limiting your ability to perform daily activities.
Dupuytren's Contracture most commonly effects the ring and little fingers and usually progresses slowly over months or even years. Though not typically painful, it can significantly impact your hand function and quality of life.
Symptoms of Dupuytren's Contracture
Symptoms of Dupuytren's Contracture tend to develop gradually. Many people don’t notice anything is wrong until the condition has significantly progressed.
Nodules: Small, firm lumps in the palm that may feel tender early on.
Cords: Thickened tissue under the skin that may appear like a rope or string pulling the finger down.
Difficulty with daily tasks: Trouble placing the hand flat on surfaces, putting on gloves, or shaking hands.
Contracture: Fingers, especially the ring and little fingers, begin to bend toward the palm and can’t be fully straightened.
Causes of Dupuytren's Contracture
The exact cause of Dupuytren's Contracture is still not fully understood, but several contributing factors are known. It seems to be a combination of genetic and environmental triggers that lead to the thickening of connective tissue in the hand.
Contributing factors for developing Dupuytren's Contracture:
Genetics: A strong family history suggests a hereditary link.
Age: Most common in people over 50.
Gender: Men are more likely to develop it than women.
Ancestry: People of Northern European descent have a higher risk.
Lifestyle factors: Alcohol use and smoking have been linked to increased risk.
Can You Prevent Dupuytren's Contracture?
Unfortunately, there is no guaranteed way to prevent Dupuytren's Contracture, especially if you have a strong genetic predisposition. However, managing certain lifestyle choices may help reduce the risk or delay its onset.
Avoid smoking: Smoking is linked to blood vessel constriction, which may influence tissue changes.
Limit alcohol: Excessive alcohol intake may increase risk.
Control diabetes: Dupuytren's is more common in people with diabetes, so maintaining good blood sugar control may help.
Is Dupuytren's Contracture Genetic?
Yes, Dupuytren's Contracture is strongly linked to genetics. If you have a family history of the condition, you have a higher chance of developing it. It is often referred to as a hereditary condition, especially prevalent among those of Northern European ancestry.
This doesn’t mean you’re guaranteed to develop it, but you may want to keep an eye out for early signs and consult a healthcare provider if you notice symptoms.
What Helps Dupuytren's Contracture?
While Dupuytren's Contracture cannot be cured entirely, several treatments and management strategies can help maintain hand function and slow progression.
Stretching and hand therapy: Gentle exercises may improve flexibility in early stages.
Splinting: In some cases, night splints may be recommended to keep fingers extended.
Steroid injections: Can reduce inflammation in early stages.
How to Treat Dupuytren's Contracture
When the condition begins to interfere with your hand function, more active treatments may be helpful. These treatments for Dupuytren's Contracture can range from minimally invasive procedures to surgery.
Surgery (fasciectomy): In more severe cases, the thickened tissue is surgically removed.
Needle aponeurotomy: A needle is used to break the cords of tissue causing finger contraction.
Enzyme injections (collagenase): An enzyme is injected to soften and break down the cords.
What Makes Dupuytren's Contracture Worse?
Several factors may accelerate the progression or severity of Dupuytren's Contracture. Understanding these can help you avoid worsening the condition.
Ignoring symptoms: Delaying treatment can make eventual correction more difficult.
Injury to the hand: Trauma may exacerbate symptoms.
Smoking and heavy alcohol use: Both are associated with higher risk and more aggressive progression.
Do Certain Careers Make Dupuytren's Contracture More Likely?
Overuse or certain jobs have not been definitively proven to cause Dupuytren’s Contracture. While it might seem like repetitive hand use or manual labor is the culprit (especially because many people who do physical work notice the symptoms), research hasn’t confirmed a direct cause-and-effect link.
Some people used to think Dupuytren’s Contracture was mostly a problem for manual laborers because of things like hand strain or using vibrating tools. But more recent research shows it can affect anyone, no matter what kind of job they have, even people who work at desks all day. Physical work might make the symptoms show up sooner, but it doesn’t actually cause the condition. If anything, overusing your hands once Dupuytren’s has started might make it worse, but it’s not the root cause.
Making practical adjustments to your daily activities can help you maintain your independence and comfort as you manage Dupuytren's Contracture.
Modify tools and grips: Use ergonomic handles and adaptive devices for easier grip.
Stay active: Gentle hand stretches and overall fitness support circulation and mobility.
Monitor for progression: Regularly assess hand function and stay in touch with a provider.
When to See an Orthopedic Hand Specialist for Dupuytren's Contracture
If you notice any signs of finger contracture or thickened tissuein your palm, you should see a hand specialist. Early diagnosis can lead to better treatment outcomes.
Signs it’s time to see a specialist:
You can’t lay your hand flat on a table.
You notice visible cords or lumps.
Daily tasks like writing or grasping are becoming difficult.
How a Hand Specialist Diagnoses Dupuytren's Contracture
Diagnosis usually involves a physical examination. An orthopaedic hand specialist will assess the flexibility of your fingers and look for nodules or cords in the palm.
What the evaluation includes:
Tabletop test: You try to lay your hand flat on a table.
Palpation: The doctor feels for cords and nodules.
Range of motion: They assess how far you can move your fingers.
Yes, while there is no cure, Dupuytren's Contracture is treatable. With appropriate care, many people regain much of their hand function or prevent further deterioration. Early intervention is often key.
Treatment outcomes vary based on the severity of the condition and the method used. Some treatments offer lasting relief, while others may need to be repeated.
The Future with Dupuytren's Contracture
Living with Dupuytren's Contracture can be manageable with awareness and timely care. Many people continue to live active, fulfilling lives with the help of therapy, medical treatments, and modifications. Emerging therapies and surgical techniques continue to improve outcomes.
Stay informed, stay proactive, and don’t hesitate to seek help when changes begin.
What Not to Do If You Have Dupuytren's Contracture
Avoiding certain actions can help prevent further damage or worsening of the condition.
Do not ignore changes: Early symptoms matter.
Avoid forceful stretching or self-treatment: This can injure tissue.
Don’t skip follow-ups: Regular monitoring can catch progression early.
Avoid smoking and excessive alcohol: Both contribute to worsening the condition.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
At Princeton Orthopaedic Associates, your journey to better mobility and less pain doesn't end at the clinic doors. We’re thrilled to now offer Prescribe FIT, an innovative, insurance-covered virtual health coaching program that brings real, lasting change right to your home.
Whether you’re preparing for surgery, recovering from one, or simply hoping to reduce joint pain and improve your lifestyle, Prescribe FIT was made with you in mind.
What Is Prescribe FIT?
Prescribe FIT is more than just a health coaching program; it’s a partnership. You are paired with your own dedicated health coach, who works one-on-one with you to support healthier eating habits, consistent physical activity, and other simple lifestyle changes that can have a significant impact on orthopedic health.
This isn’t a one-size-fits-all solution. Your health coach will tailor each step to your unique goals, challenges, and daily routines, helping you stay motivated, on track, and supported every step of the way.
Why It Matters for Orthopaedic Health
Musculoskeletal (MSK) conditions like osteoarthritis, back pain, joint injuries, and post-surgical recovery are deeply affected by lifestyle habits. For many patients, weight loss and increased mobility are essential to reducing joint stress and chronic discomfort.
With Prescribe FIT, you can:
Alleviate daily joint pain
Improve strength and flexibility
Increase energy and stamina
Support better outcomes before and after surgery
Prevent future orthopedic issues from developing
And the best part? You do it all from the comfort of your home, with expert support just a phone call or message away.
Covered by Insurance? Yes, Really!
We believe that better health should be accessible to everyone. That’s why Prescribe FIT is covered by Medicare, Medicaid, and most major commercial insurers. Our friendly POA team will help you verify your eligibility and explain any financial responsibilities up front, so you can focus on your health, not the paperwork.
Ready to Begin?
If you’ve been told weight loss or lifestyle changes could help your orthopedic condition, but you’re unsure where to start, Prescribe FIT is the perfect place. There’s no pressure, no crash diets, no complicated gym routines. Just real, achievable goals that help you feel better, move better, and live better.
At POA, we’re always looking for ways to expand your care beyond the exam room. Prescribe FIT is one more way we’re investing in your long-term wellness, because how you heal matters just as much as where you heal.
Ask your POA provider about Prescribe FIT at your next visit, or contact us today to learn more about enrollment.
Let’s take the first step, together.
Pain After A Pop In The Knee
An ACL tear typically occurs during sudden pivoting, awkward landings, or stops, which are common in sports such as basketball, soccer, and skiing. It usually starts with a moment, an awkward pivot during a pickup basketball game, a sudden stop on the soccer field, or landing just slightly wrong after a jump. You might feel a sharp pain, instability, or hear that telltale pop. You go down, maybe hoping it’s nothing, but your knee swells, and walking becomes difficult. That’s the moment many athletes, professional, weekend warriors, or even teenagers, begin their journey with an ACL tear.
Understanding how to recognize a minor knee issue needing minimal home treatment versus what may be an ACL tear can be critical to the proper treatment and the fastest path to healing.
What Is the ACL and Why Does It Matter?
Your knee is one of the most complex joints in your body, and the ACL is one of its most important components. It plays a huge role in keeping your knee stable and allowing you to move with confidence, whether you're sprinting down a field or simply walking downstairs.
The ACL (anterior cruciate ligament) is one of the four major ligaments in your knee, connecting your thigh bone (femur) to your shinbone (tibia). Its job is to stabilize the knee, especially during rotation, pivoting, and rapid direction changes. That makes it crucial for athletes, but also important for anyone who walks, runs, or climbs stairs.
When the ACL tears, it doesn’t heal on its own. And unlike muscles, ligaments don’t regenerate well without surgical reconstruction.
ACL Tear Symptoms: What You Might Experience
If you’ve injured your knee and are wondering if it’s your ACL, you’re not alone. Knowing what symptoms to look for can help you decide whether it’s time to see a doctor or get imaging.
Here’s what people often report:
A “popping” sound or sensation at the moment of injury
Immediate pain, sometimes severe enough to stop activity
Swelling that begins within a few hours
Instability or “buckling”, especially when trying to pivot or walk
Loss of full range of motion
Some people can walk after an ACL tear, especially once swelling subsides, but the knee often feels unstable. Grade 1 (mild) tears may feel like soreness and instability under stress, but they’re rare. By two weeks post-injury, swelling may reduce, but instability often persists.
Grade 3 (Complete tear): Surgical (ACL reconstruction) 6–12 months before full return to sport
MCL Tear Recovery:
Grade 1 (mild, stretching without tearing): 1–3 weeks
Grade 2 (moderate, partial tear): 3–6 weeks with bracing and PT
Grade 3 (complete): 6–10 weeks, may involve bracing or rare surgical repair
Why you can trust us:
We have multiple highly specialized, board-certified, fellowship-trained orthopaedic surgeons.
We know that we serve people - actual humans - not random orthopaedic conditions. That drives us to compassionate care.
The world of orthpaedics is constantly evolving. Our orthopaedic surgeons are constantly evaluating new techniques, tools and methods to serve our community even better.
We provide outcome-focused treatment. We work with our patients to achieve their goals, all while developing custom treatment plans that fit our patient's lives.
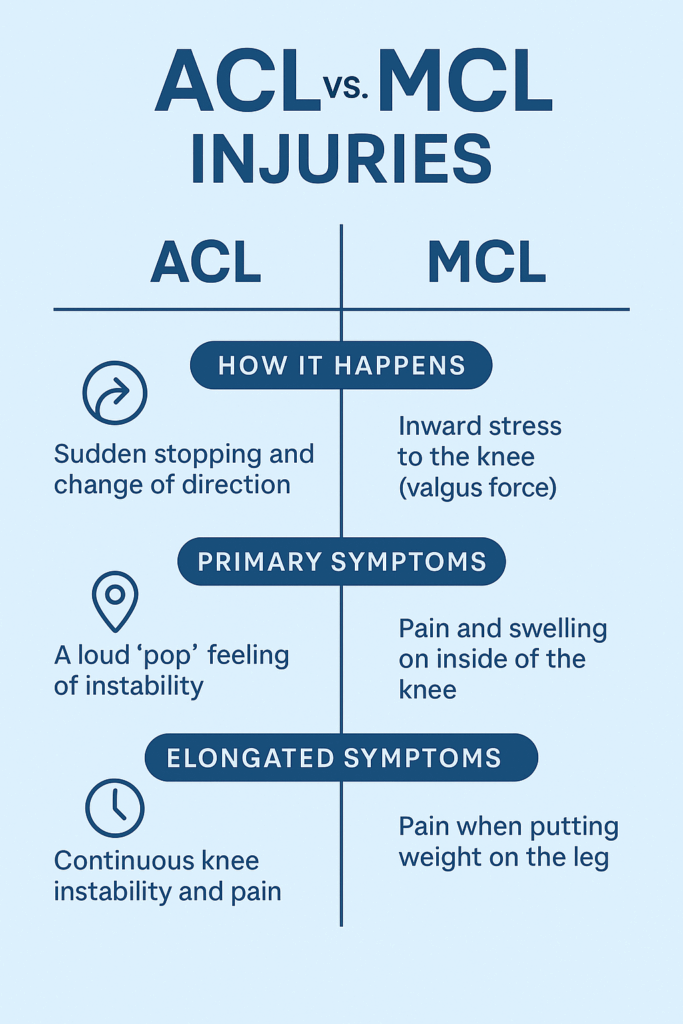
Knee injuries can be confusing because symptoms often overlap. The ACL and MCL are two different ligaments with different functions, injury mechanisms, and treatment approaches. Understanding the difference is critical for proper recovery.
Many people confuse ACL and MCL (medial collateral ligament) injuries. Here’s how an ACL tear and MCL tear differ:
ACL Tear
MCL Tear
Location
Inside the knee, central
Inside of the knee (medial side)
Mechanism
Pivoting, cutting, or landing
Direct blow to outer knee or overstretching
Sound
Often a pop
Less commonly a pop
Swelling
Fast and significant
Less severe swelling
Instability
Knee feels unstable or “gives out”
Usually more stiff than unstable
Healing Potential
Does not heal on its own
Often heals without surgery
First-line Treatment
Physical therapy or surgical reconstruction
Bracing, rest, and physical therapy
Surgery Needed?
Often required in active patients
Rarely required (unless Grade 3 + other injuries)
Return to Sport
6–12 months (after reconstruction)
4–12 weeks (depending on severity)
Key difference: An MCL tear can often heal with rest and bracing. An ACL tear usually won’t.
Can You Tear Both ACL and MCL at Once?
Yes, and this is more common than people think, especially in sports injuries. This is called a combined ligament injury and often involves the ACL, MCL, and/or meniscus. These cases require specialized surgical planning and longer rehabilitation timelines, making early diagnosis even more critical.
How to Know Which One You’ve Injured
While some clues (pain location, swelling speed, mechanism) may point toward one ligament over the other, you cannot reliably self-diagnose an ACL or MCL tear. Some people with a complete ACL tear are still able to walk or bend their knee, which can be misleading.
We recommend consulting one of our sports medicine specialists or an orthopedic knee surgeon as soon as possible. A timely and accurate diagnosis gives you the best chance of a full recovery and of avoiding chronic knee issues.
Adolescent ACL Tear vs. Adult ACL Tear
When it comes to ACL injuries, age matters. Kids and teens are still growing, and that can make treatment more complicated. What’s best for a 14-year-old soccer player may be very different from what’s recommended for a 30-year-old runner.
ACL injuries are increasing in adolescents, especially teenage athletes. The growth plates (areas of developing cartilage near the ends of long bones) in kids add complexity:
Non-surgical approaches may be prioritized in younger teens to avoid damaging growth plates.
Modified surgical techniques (like physeal-sparing procedures) are used if surgery is necessary.
Rehabilitation may need to be longer to protect future growth and return-to-play safely.
In adults, decisions are often based on lifestyle, activity level, and degree of instability.
Surgery isn't always required for an ACL tear, but it can often be recommended. Once you’ve torn your ACL, the big question is: Do you need surgery? The answer depends on your goals, age, activity level, and the nature of the tear. For some, physical therapy may be enough. For others, reconstruction is the most straightforward path back to full function. Your treatment path is specific to you, and our specialists will build a plan that meets the needs of your injury and desired recovery outcome.
Non-Surgical ACL Tear Treatment (select cases)
Mild (grade 1) sprains may recover within 3–6 weeks with rest and rehab.
For:
Low-demand lifestyle (non-athletes)
Partial tears
Older adults
No instability with daily activity
Approach:
Activity modification
Physical therapy to strengthen surrounding muscles (especially quads and hamstrings)
Bracing for certain activities
Surgical ACL Tear Treatment (Reconstruction)
Surgery may sound intimidating, but for many people, it offers the best chance at regaining full knee stability and returning to high-level physical activity. The procedure is common, safe, and continually improving.
Most active individuals, especially athletes or younger patients, choose ACL reconstruction. Here’s how it works:
Torn ACL is replaced with a graft (from your own hamstring, patellar tendon, quadriceps tendon, or a donor).
Surgery is typically minimally invasive (arthroscopic).
Recovery involves 6–12 months of guided physical therapy.
Factors influencing surgery:
Presence of other injuries (meniscus tear, cartilage damage)
Age and activity level
Desire to return to sports
Degree of instability
What Not To Do After an ACL Tear
Sometimes what you don’t do is just as important as what you do. The wrong move after an ACL tear can worsen the injury or lead to complications down the line.
Don’t ignore instability. Repeated “giving out” episodes can damage the meniscus or cartilage.
Don’t rush rehab. Returning to play too soon raises your risk of re-tear (or injuring the other knee).
Don’t skip the MRI. X-rays won’t show ligament damage. An MRI is needed to confirm the tear and check for other injuries.
Don’t rely solely on a knee brace if you're planning to return to sport, it doesn't replace ligament function.
Leaving an ACL tear untreated can lead to further joint damage, including cartilage wear or meniscus tears.
Can You Still Use Your Knee with a Torn ACL?
Some people can still walk, squat, or bend their knee shortly after tearing their ACL. However, without stability, these motions can cause further injury. If you suspect you have an ACL tear we recommend you see a orthopaedic specialist as soon as possible for a comprehensive evaluation.
Life After an ACL Tear: Hope, Patience, and Progress
An ACL tear is a detour, not a dead end. With the right care, commitment, and patience, people of all ages get back to running, jumping, and playing, often even better than before.
Tearing your ACL can feel like the end of your athletic identity, but it’s not. Thousands of people, from high school athletes to weekend hikers to pro players, successfully return to sports and active lifestyles every year.
The key is getting the right diagnosis, choosing the right treatment path for your goals, and committing to smart, structured rehab.
Diagnosis: Why You Need a POA Orthopaedic or Sports Medicine Specialist
While some symptoms can help differentiate between the two, it’s extremely difficult to diagnose knee ligament injuries accurately without imaging and specialist assessment.
Here’s why seeing a POA or orthopedic knee specialist is essential:
Physical tests (like Lachman or valgus stress test) must be performed with skill and interpreted in context.
MRI scans are required to confirm the exact ligament involved and assess associated injuries (meniscus, cartilage).
Misdiagnosis can delay proper healing. For example, treating an ACL tear like an MCL sprain could lead to long-term instability or joint damage.
Bottom Line: Always get a clinical evaluation with a knee specialist, especially if you heard a pop, felt instability, or have swelling. Don’t self-diagnose based on symptoms alone.
Meet Our Orthopaedic Knee Specialists
Can You Recover from an ACL Tear? Here’s What to Expect
Tearing your ACL may feel overwhelming, but it's not the end of your active lifestyle. Whether you're a competitive athlete or someone who just wants to move without fear, recovery is possible with the right approach. From early diagnosis and personalized treatment plans to structured rehab and return-to-play timelines, every step forward matters. Understanding your options is the first step toward getting back to what you love, with strength and confidence.
If you’re reading this, you may be worried about what’s next. Take a breath, you’re not alone. Understanding your injury is the first step toward healing. Now it’s time to take action. If you suspect an ACL tear, don’t wait. Get evaluated by a sports medicine physician or orthopedic specialist. Early diagnosis means earlier healing and a better chance of getting back to doing what you love.
ACL Tear vs. Meniscus Injury: Key Differences at a Glance
While both ACL and meniscus injuries are common in athletes and active individuals, they are very different in structure, symptoms, and recovery needs. Knowing the distinctions can help guide proper diagnosis and treatment.
How an ACL Tear and Meniscus Tear Happen
ACL Tear:
Typically from a sudden pivot, change in direction, or awkward landing
Often non-contact, though can also result from trauma
Common in sports like soccer, basketball, skiing
Meniscus Tear:
Often caused by twisting the knee while the foot is planted
Can occur with or without an ACL tear
May result from degeneration in older adults or a sharp movement in younger athletes
Primary (Immediate) Symptoms
Symptom
ACL Tear
Meniscus Tear
Popping Sound
Very common
May occur, but less dramatic
Swelling
Rapid (within hours)
Gradual (over 24–48 hours)
Instability
Knee may "give out"
Usually feels stable
Pain Location
Deep or central knee
Side or back of knee (depending on tear location)
Mobility
Loss of motion due to swelling and instability
May still walk, but discomfort with twisting/squatting
Prolonged/Chronic Symptoms (If Left Untreated)
Symptom
ACL Tear
Meniscus Tear
Knee Giving Out
Frequent instability, especially during pivoting
Rarely unstable
Locking or Catching
Uncommon
Very common — knee may catch or lock during motion
Grinding or Clicking
Occasionally
Common, especially with movement
Degeneration Risk
Higher if combined with meniscus injury
Increases risk of arthritis over time
Return to Activity
Difficult without surgery for active individuals
Sometimes possible without surgery, depending on severity and tear location
A meniscus tear often presents with joint line tenderness and mechanical symptoms (like locking), while an ACL tear leads to feelings of instability and swelling shortly after injury. However, since both can coexist, and symptoms can overlap, accurate diagnosis with an MRI and specialist evaluation (by a POA or orthopedic physician) is essential. Read more about meniscus tears.
Quick Overview
ACL
Meniscus
Function
Stabilizes the knee
Cushions and supports joint movement
Injury Type
Ligament
Cartilage
Instability?
Yes
Rarely
Locking
Rare
Common
Needs Surgery
Often (for active patients)
Sometimes, depending on tear type
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.