We get it. We like our acronyms! Orthopaedic Surgeons, and doctors in general, often go around saying groups of letters as if everyone is going to get it.
That’s why we’ve created a comprehensive list to serve as a clear and reliable reference for our patients. Whether you’re reviewing test results, discussing a diagnosis with your physician, or reading about your recovery plan, this list can help you make sense of the medical language being used. Our goal is to empower patients with knowledge so that every conversation about your health is less intimidating and more productive.
Acronym
Full Title
Description
MD
Doctor of Medicine
Completed allopathic medical training. Focuses on traditional biomedical model and is licensed for full scope medical and surgical practice.
DO
Doctor of Osteopathic Medicine
Completes the same training as MDs with added emphasis on holistic care and musculoskeletal system. Licensed for full medical and surgical practice in the U.S.
PA-C
Physician Assistant, Certified
Graduate-level provider trained in diagnosis, treatment, and minor surgery. Works under physician supervision but can prescribe and manage care.
NP
Nurse Practitioner
Advanced practice registered nurse with graduate-level training. Provides diagnosis, treatment, and prescribing, often with a holistic emphasis.
DNP
Doctor of Nursing Practice
Highest clinical nursing degree with focus on evidence-based practice and leadership. Functions as an NP but with expanded academic and clinical training.
CRNA
Certified Registered Nurse Anesthetist
Advanced practice nurse specializing in anesthesia. Provides anesthesia independently or alongside anesthesiologists in surgery and trauma settings.
Bone & Joint Conditions
BMD – Bone Mineral Density: Measurement of bone strength using imaging (DEXA scan). Helps diagnose osteoporosis and fracture risk. Essential for long-term bone health monitoring.
CTS – Carpal Tunnel Syndrome: Compression of the median nerve at the wrist. Causes numbness, tingling, and hand weakness. Often treated with splints, injections, or surgery.
OA – Osteoarthritis: Degenerative joint disease due to cartilage breakdown. Causes pain, stiffness, and reduced range of motion. Common in hips, knees, and hands.
RSI – Repetitive Strain Injury: Overuse injury to muscles, tendons, or nerves. Common in wrists, elbows, and shoulders. Preventable with ergonomic adjustments.
Fractures & Fixation
FNF – Femoral Neck Fracture: Break in the neck of the femur, common in elderly after falls. High risk of complications due to disrupted blood supply. Treated with screws, arthroplasty, or hemiarthroplasty.
Fx / Frx – Fracture: Break in a bone. Classified by pattern, location, and stability. May require casting, fixation, or surgery.
DHS – Dynamic Hip Screw: Implant system for stabilizing femoral neck or intertrochanteric fractures. Allows controlled compression during healing. Inserted surgically into the femur.
SHS – Sliding Hip Screw: Similar to DHS, used for hip fracture stabilization. Provides controlled movement as the fracture heals. Widely used in orthopaedic trauma.
IMN – Intramedullary Nail: Rod placed inside bone marrow canal for fracture stabilization. Common in long bone fractures. Provides strong internal fixation.
CMN – Cephalomedullary Nail: Type of intramedullary nail extending into the femoral head. Stabilizes proximal femur fractures. Often chosen for unstable hip fractures.
ORIF – Open Reduction Internal Fixation: Surgical repair of fractures using plates, screws, or rods. “Open reduction” means exposing the bone surgically. “Internal fixation” stabilizes it from inside.
Ex-fix – External Fixator: Frame with pins/wires inserted into bone through skin. Stabilizes fractures or corrects deformities externally. Used in severe trauma or infection cases.
Arthroplasty & Joint Replacement
THA – Total Hip Arthroplasty: Complete hip replacement with artificial components. Relieves pain from arthritis or fractures. Improves mobility and quality of life.
TKA – Total Knee Arthroplasty: Replacement of the knee joint with artificial implants. Used for end-stage arthritis or deformity. Restores function and reduces pain.
TSA – Total Shoulder Arthroplasty: Replacement of the shoulder joint with prosthesis. Improves motion and relieves pain. Used for arthritis or severe fractures.
RSA – Reverse Shoulder Arthroplasty: Shoulder replacement where ball and socket are reversed. Provides stability when rotator cuff is deficient. Useful in complex shoulder conditions.
DFR – Distal Femoral Replacement: Prosthetic replacement of lower femur. Used in severe fractures or tumors. Restores knee joint stability and function.
Neuro & Physical Exam Terms
DTR – Deep Tendon Reflexes: Involuntary muscle contractions when tendon is tapped. Used to assess nerve and spinal cord function. Commonly tested in knees and ankles.
SILT – Sensation Intact to Light Touch: Exam finding documenting preserved skin sensation. Indicates intact nerve function. Common in trauma assessments.
AIN – Anterior Interosseous Nerve: Branch of the median nerve controlling thumb/index finger flexion. Injury causes weakness in pinch grip. Tested with “OK sign.”
PIN – Posterior Interosseous Nerve: Branch of the radial nerve controlling finger extension. Injury causes finger drop. Often injured in forearm trauma.
Motion & Weight Bearing
FROM – Full Range of Motion: Joint can move normally in all planes. Indicates absence of stiffness or contracture. Often documented in rehab notes.
PROM – Passive Range of Motion: Movement performed by examiner without patient effort. Tests joint flexibility and stiffness. Important in rehab and post-op recovery.
AROM – Active Range of Motion: Movement performed by patient voluntarily. Assesses muscle strength and function. Limited in cases of weakness or pain.
NWB – Non-Weight Bearing: Patient must not put weight on injured limb. Requires crutches, walker, or wheelchair. Standard after major fractures or surgery.
PWB – Partial Weight Bearing: Patient may put limited weight on limb. Usually specified as percentage (e.g., 25%). Step-down progression in rehab.
TTWB – Toe Touch Weight Bearing: Only toes lightly touch the ground for balance. No real weight through limb. Transition stage before partial weight bearing.
FFWB – Foot Flat Weight Bearing: Patient may rest entire foot but not load limb. Intermediate between TTWB and PWB. Used for gradual progression.
WBAT – Weight Bearing as Tolerated: Patient bears as much weight as comfortable. Limited only by pain. Common after stable fracture fixation.
Trauma & Mechanism
APC – Anterior Posterior Compression: Pelvic fracture pattern from front-to-back force. Causes pelvic instability and bleeding risk. Often from high-energy trauma.
LC – Lateral Compression: Pelvic fracture pattern from side-to-side force. Stability varies with severity. Common in vehicle or crush injuries.
GLF – Ground-Level Fall: Fall from standing height. Common cause of hip and wrist fractures in elderly. Often signals osteoporosis or frailty.
GSW – Gunshot Wound: Penetrating trauma from firearm. May involve bone, nerves, and vessels. Requires multidisciplinary care.
Materials
Provider & Professional Acronyms
Physicians
MD – Doctor of Medicine: Completed allopathic medical training. Focuses on traditional biomedical model. Trained in surgery, prescribing, and full scope practice.
DO – Doctor of Osteopathic Medicine: Completes same training as MD with additional focus on holistic care and musculoskeletal system. Uses osteopathic manipulative treatment (OMT). Licensed for full practice in the U.S.
Additional Physician Types
PA-C – Physician Assistant, Certified: Graduate-level medical provider trained in diagnosis, treatment, and minor surgery. Works under physician supervision. Can prescribe medication.
NP – Nurse Practitioner: Advanced practice registered nurse with graduate-level training. Provides diagnosis, treatment, and prescribing. Often emphasizes preventive and holistic care.
DNP – Doctor of Nursing Practice: Highest clinical degree for nursing. Focuses on leadership, evidence-based practice, and advanced clinical skills. Functions as an NP with expanded academic training.
Nursing & Allied Health
RN – Registered Nurse: Provides patient care, medication administration, and coordination. Licensed after nursing degree and national exam. Backbone of hospital and surgical teams.
LPN – Licensed Practical Nurse: Provides basic patient care under RN supervision. Training shorter than RN. Common in rehab and outpatient settings.
CNA – Certified Nursing Assistant: Assists patients with daily living tasks. Works under nurses’ supervision. Provides vital bedside support.
CRNA – Certified Registered Nurse Anesthetist: Advanced practice nurse specializing in anesthesia. Provides anesthesia independently or with anesthesiologists. Critical in surgery and trauma care.
Therapy & Rehabilitation
PT – Physical Therapist: Doctorate-level provider specializing in mobility, strength, and rehab. Designs exercise programs for recovery. Critical after surgery or injury.
DPT – Doctor of Physical Therapy: Doctoral degree in physical therapy (entry-level in U.S.). Focuses on evidence-based rehab care. Equivalent to PT but emphasizes doctoral training.
OT – Occupational Therapist: Helps patients regain independence in daily activities. Focuses on upper extremity function and adaptive strategies. Important post-surgery or after injury.
COTA – Certified Occupational Therapy Assistant: Works under OT supervision. Delivers therapy exercises and training. Provides hands-on patient support.
ATC – Athletic Trainer, Certified: Specializes in sports medicine, injury prevention, and rehab. Works with athletes and orthopaedic teams. Provides on-field and clinical support.
Surgical & Training Roles
FA – First Assistant: Assists primary surgeon with exposure, suturing, and technical tasks. Can be physician, PA, or NP. Enhances operative efficiency.
SA – Surgical Assistant: Supports surgeon intraoperatively with retraction, suction, and prep. May be trained staff or non-physician. Distinct from scrub nurse.
PGY-# – Post-Graduate Year: Indicates level of residency training. Example: PGY-3 = third-year resident. Determines experience and role in surgery.
MS4 – Fourth-Year Medical Student: Final year before graduation from medical school. May assist in surgery under supervision. Limited responsibilities compared to residents.
Certifications
FAAOS – Fellow of the American Academy of Orthopaedic Surgeons: Prestigious membership after board certification in orthopaedics. Indicates commitment to education and peer standards. Recognized globally in orthopaedics.
FACS – Fellow of the American College of Surgeons: Designation for surgeons meeting rigorous professional standards. Shows commitment to ethical and skilled surgical practice. Used across multiple specialties.
Understanding and Managing Hand Cramps
Quick overview
Hand cramps are sudden, involuntary squeezes of the muscles in your hand or fingers. They can happen during activity or at rest and often respond to simple measures, but sometimes they point to an underlying issue that needs professional care.
What Are Hand Cramps?
A hand cramp is a tight, often painful contraction of one or more hand muscles that you cannot relax immediately. They usually happen without warning and can last from a few seconds to several minutes.
Squeezing or knotting feeling in the palm or fingers
Difficulty opening the hand while the muscle is tight
Sometimes a visible twitch or hard lump under the skin
Common Triggers for Hand Cramps
Several everyday factors can make hand cramps more likely. Often more than one factor is involved.
Muscle overuse from repetitive tasks like typing, sewing, or gripping tools
Muscle fatigue after unusual or prolonged hand activity
Dehydration or mineral imbalances such as potassium, magnesium, or calcium can contribute in some contexts, but not all cramps require supplementation
Nerve irritation or compression in the wrist or forearm
Certain medications or medical conditions that affect nerves or muscles
What a Hand Cramp Feels Like
Hand cramps can vary from a mild tightness to a painful spasm. They may affect one finger, several fingers, or the whole hand. Symptoms often come on suddenly and can interfere with normal hand use until the muscle relaxes.
Sharp or aching pain during the spasm
Stiffness or reduced grip strength afterwards
Occasional tingling if a nerve is involved
Immediate Steps to Ease a Cramp
If a cramp starts, try these simple measures to help the muscle relax. These steps are safe for most people and often work quickly.
Stop the activity that triggered it and gently stretch the affected finger or hand
Massage the tight muscle using light pressure to increase blood flow
Apply a warm compress if the muscle feels tight, or cold if there is sharp pain after activity
Drink water; if dehydration or electrolyte imbalance is suspected, seek clinician guidance and appropriate testing; routine potassium or magnesium supplementation for isolated hand cramps is not universally recommended
Try shaking your hand or opening and closing the fingers slowly to help the spasm pass
Note: If cramps happen frequently, or are severe, it is important to get a medical review to find the cause.
Longer Term Strategies to Prevent Recurrence
Preventing hand cramps often means addressing how you use your hands and caring for overall muscle and nerve health. Small daily changes can reduce episodes significantly.
Take regular short breaks during repetitive tasks to rest and stretch
Use ergonomic tools and adjust your workspace to reduce strain on the wrist and hand
Strengthen hand and forearm muscles with guided exercises if recommended by a therapist
Stay hydrated and eat a balanced diet that includes minerals important for muscle function
Consider splinting at night if cramps wake you from sleep or if a nerve problem is suspected
When to See a Doctor
See a clinician if cramps are persistent, frequent, worsening, occur at rest without clear triggers, or are accompanied by numbness and weakness. Those signs may indicate a nerve or systemic issue that needs evaluation.
Who Can Help
Specialist
When to Choose
Notes
Primary Care Provider
First evaluation, blood tests, medication review
Good starting point to rule out common causes
Orthopaedic Hand Specialist
Suspected structural or nerve problems in the hand or wrist
Helps correct movement patterns and build hand endurance
Neurologist
Frequent cramps with weakness or other neurological signs
Assesses nerve disorders and coordination
Treatment Options Your Specialist May Discuss
Treatment depends on the cause. Many people improve with conservative measures. In select cases, targeted therapies may be recommended.
Activity modification and ergonomic changes
Guided hand and forearm exercise programs with a therapist
Medication review and correction of electrolyte or metabolic issues
Botulinum toxin injections are not standard for routine hand cramps. They are generally considered only in rare focal dystonias or specific nerve related conditions, and carry risks such as focal weakness
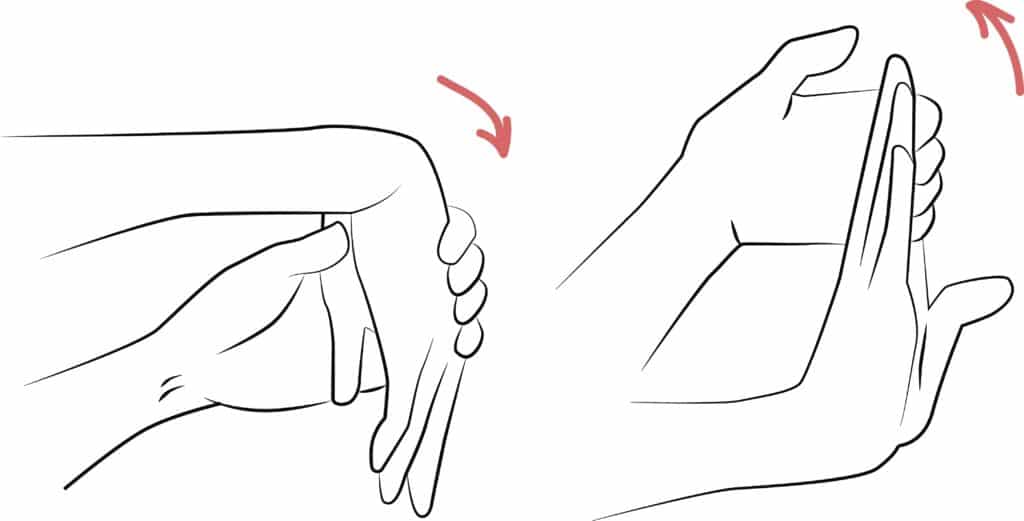
Simple Hand Stretches You Can Try
These gentle stretches may reduce tightness and build resilience. Stop if they cause sharp pain and check with a clinician if you have an injury.
Finger extension: gently bend the fingers back with the other hand and hold for 15 to 30 seconds
Thumb stretch: pull the thumb away from the palm and hold for 15 seconds
Wrist flexor stretch: straighten the arm, bend the wrist down with the palm facing out, and hold
How Long Until I Feel Better?
Recovery varies by cause and how soon you begin appropriate care. Many people improve within days when the issue is temporary. If cramps come from nerve compression or a chronic condition, recovery may take weeks to months with therapy and targeted treatment.
Typical Pattern
Timeframe
What Helps
Acute, activity related
Days to weeks
Rest, hydration, stretching
Recurrent with overuse
Several weeks
Ergonomic changes, therapy
Nerve-related (peripheral nerve compression) or other nerve-related causes
Weeks to months
Specialist evaluation and targeted care
Living With Occasional Hand Cramps
Most people can manage occasional cramps with simple self-care and small changes to daily routines. If cramps limit your work or hobbies, we can help find the right plan so you can stay active and comfortable.
If your cramps are persistent or troubling, schedule an exam with one of our hand specialists. We will review your history, examine your hand, and recommend tests or therapy if needed. Together we will create a plan tailored to your needs.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
Understanding Tylenol, Advil, and Aleve: A Parent’s Guide
A Quick Note: When it comes to over-the-counter medicine, we highly encourage you to talk to your doctor about what you are using or plan to use. It's not a good idea to take advice about medicine on the internet without consulting a medical professional. The information here is designed to give you a great overview of the differences, the main effects, and why or how they work. This is not intended to replace actual medical advice!
When your child has pain or a fever, it’s common to reach for over-the-counter medicine. But which one is best—Tylenol, Advil, or Aleve? Each works differently in the body, has different age guidelines, and comes with important safety points. This guide walks you through what each option does, how long it lasts, and when it may be appropriate so you can make the safest choice.
Key Differences at a Glance
Brand
Active Ingredient
Category
Main Effects
Tylenol
Acetaminophen
Analgesic / Antipyretic
Reduces pain and fever, but not inflammation
Advil / Motrin
Ibuprofen
NSAID
Reduces pain, fever, and inflammation
Aleve
Naproxen
NSAID
Reduces pain, fever, and inflammation; lasts longer per dose
Both Advil and Aleve are NSAIDs, which are especially helpful when swelling is part of the problem. Tylenol is not an NSAID, but it’s effective for lowering fever and easing pain without affecting inflammation.
Age Guidelines and Surgery Considerations
Tylenol can be used in infants (consult a doctor for recommended dose), and in most cases it may be given up until the time of surgery unless your surgeon advises otherwise.
Advil is not recommended for children younger than 6 months. Families should follow their surgeon’s guidance on timing before surgery—many ask families to stop ibuprofen about 3 days beforehand, but instructions can vary.
Aleve (OTC naproxen) isn’t recommended for children under 12 unless a clinician specifically advises it. Prescription naproxen may sometimes be used for pediatric conditions under physician supervision.
Safety Tips Every Parent Should Follow
Always measure carefully. Use the provided cup, dropper, or syringe. Kitchen spoons are not accurate.
Check every label. Many cold or flu medicines already include acetaminophen or an NSAID. Doubling up can cause harm.
Keep a log. Writing down the time of each dose helps prevent giving medicine too soon.
Consider health conditions. If your child has liver disease, consult their clinician before giving acetaminophen; it’s contraindicated in severe or active liver disease. Children with kidney or stomach issues may need to avoid NSAIDs.
Stay hydrated. Ibuprofen and naproxen are not recommended if your child is dehydrated because of the risk to the kidneys.
Store medicines safely. Keep them in original containers, out of reach, with caps closed tightly.
Which One Should You Choose?
If your child has swelling from an injury, an NSAID like Advil or Aleve may help. If you’re treating pain or fever without swelling, Tylenol is often a safe choice. Some families alternate Tylenol with an NSAID to avoid exceeding safe limits for either drug, but this should only be done under your doctor’s guidance.
When to See an Orthopaedic Specialist
Pain lasts for more than a few days or keeps returning.
You notice swelling, warmth, or stiffness in a joint.
Your child avoids using the limb or can’t put weight on it.
Over-the-counter medicine doesn’t improve symptoms.
Our team can help you understand what’s behind the pain, make safe choices about medicines, and design a plan that includes activity, rest, and recovery strategies.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
Why Does My Knee Pop? Common Causes and When to Get Help
Learn why knees sometimes pop, when it’s usually harmless, and when it may signal a problem. Common causes include gas bubbles or tendons snapping, but popping can also point to joint issues. Explore simple at-home steps that may help, and know when it’s time to see a clinician.
If you hear occasional popping without pain, it is usually not serious. But if popping comes with pain, swelling, instability, or locking, you should seek evaluation so we can find the cause and plan treatment.
Quick Overview: What This Post Covers
What makes knees pop.
How to tell harmless popping from trouble.
Simple self-care and when to see a specialist.
Tests and treatments your clinician may use.
How we approach diagnosis and recovery at Princeton Orthopaedic Associates.
Common, Usually Harmless Causes of Knee Popping
Sometimes popping is simply noise from normal joint movement. A few common benign reasons include:
Gas bubbles forming and popping inside the joint fluid, which can create a cracking sound
Tendons or ligaments snapping briefly as they shift over bone when the joint moves
Rough surfaces rubbing in a joint with age-related wear; osteoarthritis can also have inflammatory flares and management depends on symptoms and function
Painless popping alone is not known to cause arthritis; however, if popping is accompanied by pain, swelling, instability, or limits on function, you should have it evaluated.
When Popping May Mean a Problem
Popping that comes with other symptoms may point to an underlying injury. Watch for these signs:
Sharp or persistent pain at the time of popping
Visible swelling or the knee feeling hot
A feeling that the knee gives way, locks, or will not fully bend or straighten
Pain or instability that limits walking or daily activities
Those symptoms suggest we should examine the joint to look for cartilage injuries, meniscal tears, ligament strain, loose fragments, or significant joint inflammation.
Emergency or Urgent Signs
If any of the following occur after a pop, get urgent or emergency care rather than waiting for a routine appointment:
A loud pop during an injury followed by immediate swelling and inability to bear weight
Visible deformity or suspected patellar dislocation
The knee is locked and you cannot fully straighten it - true mechanical locking
Severe pain after trauma or when a fracture is suspected
A hot, very painful swollen knee with fever or chills, or a swollen painful knee in someone who is immunocompromised - possible septic arthritis
What Might Be Causing Painful Popping?
Several common issues can cause painful popping. These include damage to soft tissues, cartilage problems, and mechanical irritation around the joint.
Meniscal tears. A torn meniscus can catch or lock and may produce a pop with pain.
Ligament sprains. A sudden twist or direct blow can cause ligament stretching and an audible pop.
Patellar tracking issues and patellar instability or dislocation. If the kneecap moves unevenly or subluxes, you may feel or hear snapping and experience pain.
Loose bodies or osteochondral injury. Cartilage or bone fragments can catch in the joint and cause painful popping or locking.
Cartilage wear. As cartilage thins with age or injury, joint surfaces can make noise and become painful.
How We Evaluate Popping Knees
Your clinician will take a careful history and perform a focused exam to check motion, stability, and areas of tenderness. That helps narrow down likely causes.
Imaging and tests are selected based on the history and exam. X-rays are often first-line after trauma to assess for fracture and alignment; X-rays do not show soft tissues. MRI is ordered when the exam or history suggest soft tissue injury such as meniscus or ligament tears, cartilage damage, or when mechanical symptoms persist. Ultrasound can be useful for dynamic snapping and for evaluating superficial tendon or bursal problems.
Test
What it shows
X-ray
Bone alignment, fracture, and evidence of arthritis; does not show soft tissues
MRI
Soft tissues like meniscus, ligaments, and cartilage; used when exam or history suggest soft tissue injury or persistent mechanical symptoms
Ultrasound
Tendon or bursa irritation near the knee and useful for dynamic snapping
At-home Steps You Can Try First
If popping is mild and not accompanied by the concerning signs above, try conservative care while watching symptoms. Small changes often help.
Rest from the activity that triggers the sound for a few days
Ice the area for 10 to 15 minutes if there is pain or swelling
Over-the-counter nonsteroidal anti-inflammatory drugs may reduce pain; avoid NSAIDs if you have a history of gastrointestinal ulcers or bleeding, kidney disease, are taking blood thinners, are in late pregnancy, or have an NSAID allergy. If NSAIDs are not appropriate, consider acetaminophen after checking with your provider
Start gentle strengthening and mobility work for hips, quads, and hamstrings; a physical therapist can guide this
When You Should Schedule an Exam
Contact us for an evaluation if you have persistent pain, swelling, catching or locking, repeated giving way, or if symptoms prevent daily tasks. Early assessment helps us treat the cause and reduce the chance of longer term issues.
Who to See at Princeton Orthopaedic Associates
Specialty
Why you would see them
Sports Medicine
Non surgical evaluation for tendon, ligament, and meniscal problems
Orthopaedic Surgeon
Persistent mechanical symptoms or when surgery may be needed
Physical Therapist
Rehabilitation to improve strength, control, and movement patterns
What to Expect from Treatment
Treatment depends on the diagnosis. Many causes improve with a planned rehab program that reduces pain, restores motion, and strengthens supporting muscles. When structural damage is severe, surgical options may be discussed.
Conservative care first: activity modification, medication, targeted therapy
Procedures: injections may help for persistent inflammation
Surgery: reserved for clear mechanical problems or unresolving structural injury
If you want to discuss symptoms, we make it easy to schedule an exam. A focused visit helps us determine what is normal and what needs treatment so you can get back to your routine with confidence.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.