Understand your diagnosis and all treatment options.
Review the benefits, risks, and alternatives with your provider.
Follow all preoperative instructions regarding medications, diet, and fluid intake.
Be aware of what happens during the procedure and the safety checks involved.
Arrange for a ride home and prepare your space for a comfortable recovery.
Begin gentle movement and prescribed exercises on schedule.
Call your provider immediately if you experience any warning signs.
Understanding Your Knee Pain
Your knees support you through every step, bend, and climb. Over time, injuries or the natural wear of daily life can lead to pain, swelling, or a feeling of instability. If these symptoms begin to limit the activities you love, your orthopaedic surgeon may suggest knee arthroscopy—a minimally invasive procedure that uses small incisions to look inside the joint and treat the problem.
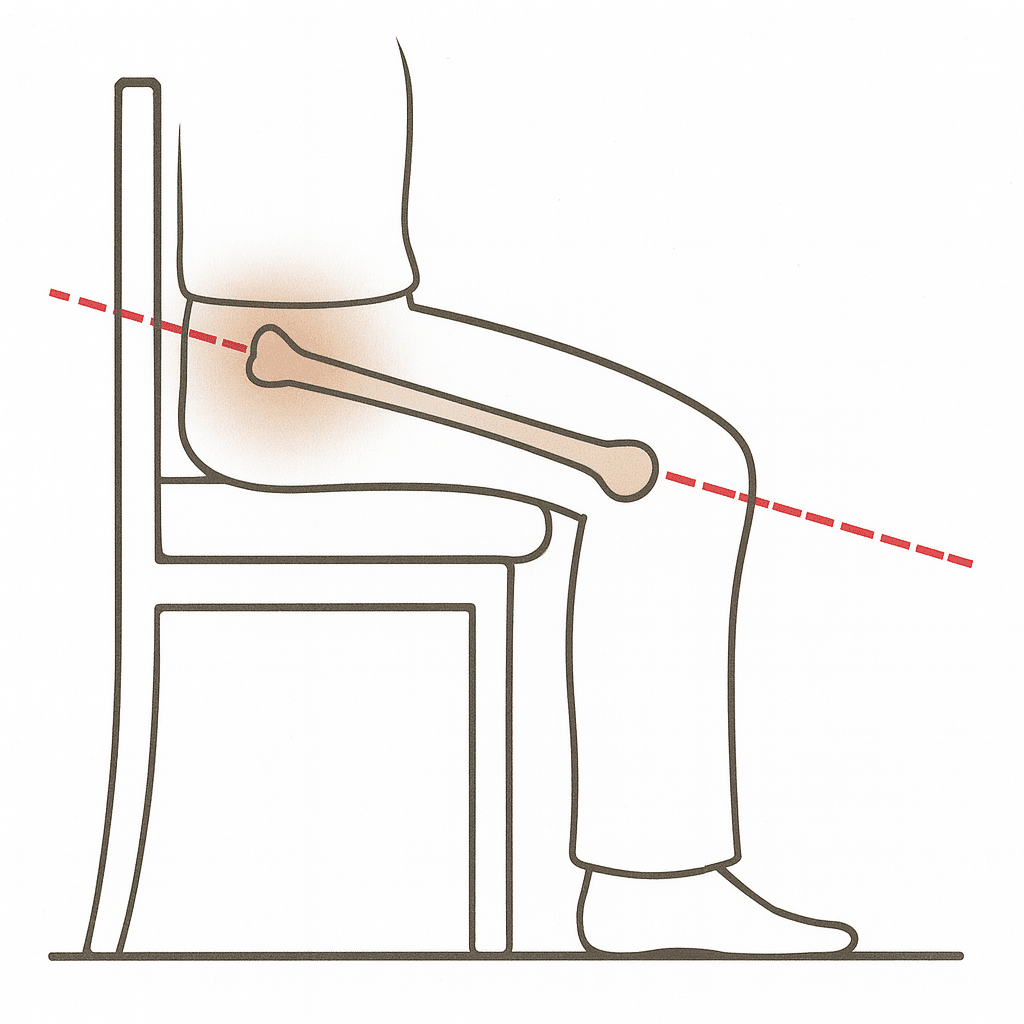
How the Knee Joint Works
The knee is a complex hinge joint where your thigh bone (femur) and shin bone (tibia) meet. A C-shaped cushion of cartilage called the meniscus sits between these bones to absorb shock. The ends of the bones, along with the back of the kneecap (patella), are coated with a smooth, slick surface called articular cartilage, which allows the joint to glide comfortably. A network of muscles, tendons, and ligaments surrounds the joint to provide strength and stability.
Is Knee Arthroscopy Right for You?
To get an accurate diagnosis, your care team may order imaging tests like an X-ray or an MRI (magnetic resonance imaging). These tests can reveal issues in the soft tissues like ligaments and cartilage, as well as in the bones themselves. Arthroscopy can then be used to confirm what the images suggest and often allows your surgeon to treat the issue during the same procedure.
You and your provider will review the expected benefits and possible risks of arthroscopy. You will also discuss alternatives, which may include medications, physical therapy, activity changes, or wearing a brace. Be sure to ask every question on your mind so you feel informed and confident in your decision.
Your Knee Arthroscopy Procedure
What to Expect on Surgery Day
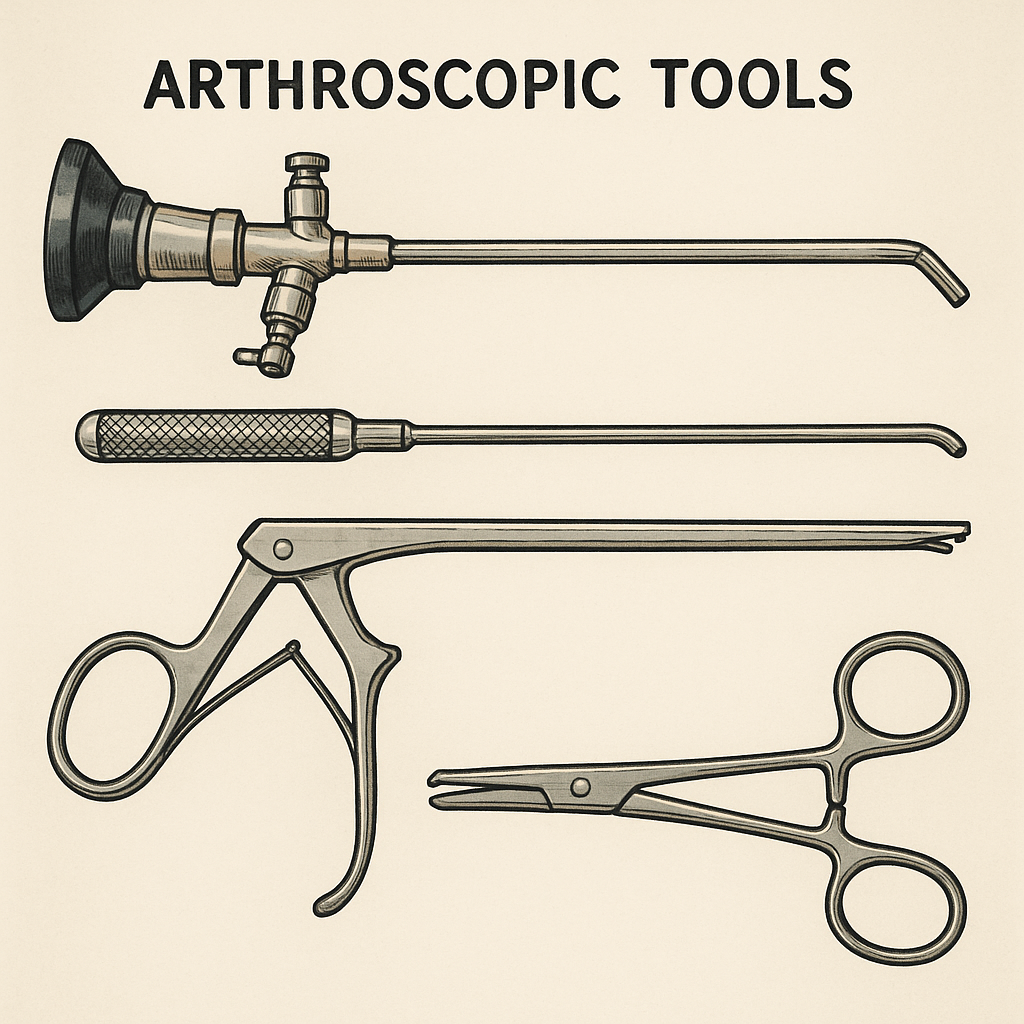
The Procedure: Arthroscopy allows the surgeon to see inside your knee using a thin, lighted camera called an arthroscope. The camera sends live images to a monitor, which guides the precise surgical tools inserted through separate small incisions. This approach allows the surgeon to diagnose and treat many knee problems through incisions that are typically less than an inch long.
Preparing: Before the procedure, inform your surgeon about all the medications and supplements you are taking. You may need to stop some of them ahead of time. You will also be instructed to stop eating and drinking for a set period to ensure your stomach is empty for anesthesia.
The Day of Surgery: On the day of surgery, your team will perform several routine safety checks, including marking the correct knee and confirming your identity and the planned procedure. Anesthesia will keep you comfortable and free from pain. The surgeon then makes two or three small incisions (called portals), places the scope through one, and inserts instruments through the others. Sterile fluid is used to gently expand the joint, improving visibility and helping the surgeon work accurately.
Risks and Possible Complications
Knee arthroscopy is a widely used and very safe procedure. However, like any surgery, it carries some risks. These may include:
Bleeding, infection, or blood clots
Stiffness or ongoing knee pain
Injury to blood vessels, nerves, or skin around the knee
Damage to cartilage, the meniscus, or ligaments
The need for additional surgery
Other specific risks as discussed by your surgeon
Common Conditions Treated with Arthroscopy
Arthroscopy can address a variety of common knee problems:
A Healthy Knee
The Problem: Repeated squatting or a sudden twist can tear the meniscus. This may cause pain or swelling, and your knee may catch or lock when you move.
The Solution: Torn tissue on the inner portion of the meniscus is often trimmed away (a meniscectomy). Tears near the outer edge, which has a better blood supply, may be repaired with sutures.
Meniscus Tears
The Problem: Repeated squatting or a sudden twist can tear the meniscus. This may cause pain or swelling, and your knee may catch or lock when you move.
The Solution: Torn tissue on the inner portion of the meniscus is often trimmed away (a meniscectomy). Tears near the outer edge, which has a better blood supply, may be repaired with sutures.
ACL Tear
The Problem: A sudden pivot, cut, or awkward landing can tear the ACL. Patients often report a “pop,” rapid swelling within hours, and instability with pivoting or cutting.
The Solution: Low-demand or partial tears may be managed with structured rehab and bracing. Symptomatic complete tears, especially in patients returning to sports, are typically treated with arthroscopic ACL reconstruction using a tendon graft; primary ACL repair is reserved for select tears.
Cartilage Wear
The Problem: Articular cartilage can wear down, and loose pieces can float inside the joint. You may notice pain, stiffness, or a grinding sensation.
The Solution: The surgeon can remove loose fragments that irritate the joint to reduce catching and pain, and smooth down damaged cartilage surfaces.
Patella (Kneecap) Issues
The Problem: Articular cartilage can wear down, and loose pieces can float inside the joint. You may notice pain, stiffness, or a grinding sensation.
The Solution: The surgeon can remove loose fragments that irritate the joint to reduce catching and pain, and smooth down damaged cartilage surfaces.
Your Recovery at Home
Immediately After Surgery
When the procedure is finished, your small incisions will be closed and covered. In the recovery room, your knee will be bandaged, iced, and elevated to limit swelling. You will receive pain medication and be monitored by a nurse until it is safe to go home. Anesthesia and pain medicine can make you drowsy, so you must arrange for an adult to drive you home.
Caring for Your Knee
Follow your surgeon’s instructions carefully to ensure a smooth recovery. Key steps include:
Elevate your leg above the level of your heart as much as possible to reduce pain and swelling.
Ice your knee for 20-30 minutes several times a day for the first few days. Wrap the ice pack in a thin towel to protect your skin.
Keep incisions dry. Shower only when your provider says it is safe, and cover your leg with plastic to keep the bandages dry.
Manage weight-bearing. You may go home with crutches. Follow your weight-bearing directions carefully so your knee can heal properly.
Exercises for a Strong Recovery
Oftentimes, physical therapy is prescribed. But at home, you can work on many of the following.
Gentle movement is critical for healing. Your provider or physical therapist will guide you through a plan to restore motion and strength. Start these simple motions as soon as you are told it is safe to improve blood flow and help prevent blood clots.
Ankle Pumps: Point your foot down, then flex it up. Move your foot in circles several times throughout the day.
Quadriceps Sets: While lying down, tighten the muscles on the front of your thigh and press the back of your knee toward the surface. Hold for 5 to 10 seconds, then relax. Repeat as directed.
Straight Leg Raises: Lying down, keep your knee straight and lift your leg 8 to 12 inches off the surface. Hold for 5 seconds, then lower slowly. Repeat as directed.
When to Call Your Provider
Contact your provider’s office right away if you notice any of the following:
Fever of 100.4° F (38° C) or higher
Pain that does not improve with medication and rest
Swelling that does not improve with elevation and icing
Increased redness, warmth, or drainage from the incision sites
Bleeding that soaks through your bandages
New or worsening numbness in your leg or foot
Severe nausea or vomiting
Returning to Your Activities
Recovery time varies based on your specific procedure, the condition of your knee, and your overall health. Many people with desk jobs can return to work in about one week. Jobs that require prolonged standing or heavy activity may require more time off. With consistent effort in your rehabilitation, most people can return to their normal active lifestyle within one to two months.
Knee arthroscopy is a powerful tool for diagnosing and treating the cause of your knee pain. By preparing as instructed and following your post-operative plan closely, you give yourself the best chance of returning to your activities with less pain and improved function.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
We get it. We like our acronyms! Orthopaedic Surgeons, and doctors in general, often go around saying groups of letters as if everyone is going to get it.
That’s why we’ve created a comprehensive list to serve as a clear and reliable reference for our patients. Whether you’re reviewing test results, discussing a diagnosis with your physician, or reading about your recovery plan, this list can help you make sense of the medical language being used. Our goal is to empower patients with knowledge so that every conversation about your health is less intimidating and more productive.
Acronym
Full Title
Description
MD
Doctor of Medicine
Completed allopathic medical training. Focuses on traditional biomedical model and is licensed for full scope medical and surgical practice.
DO
Doctor of Osteopathic Medicine
Completes the same training as MDs with added emphasis on holistic care and musculoskeletal system. Licensed for full medical and surgical practice in the U.S.
PA-C
Physician Assistant, Certified
Graduate-level provider trained in diagnosis, treatment, and minor surgery. Works under physician supervision but can prescribe and manage care.
NP
Nurse Practitioner
Advanced practice registered nurse with graduate-level training. Provides diagnosis, treatment, and prescribing, often with a holistic emphasis.
DNP
Doctor of Nursing Practice
Highest clinical nursing degree with focus on evidence-based practice and leadership. Functions as an NP but with expanded academic and clinical training.
CRNA
Certified Registered Nurse Anesthetist
Advanced practice nurse specializing in anesthesia. Provides anesthesia independently or alongside anesthesiologists in surgery and trauma settings.
Bone & Joint Conditions
BMD – Bone Mineral Density: Measurement of bone strength using imaging (DEXA scan). Helps diagnose osteoporosis and fracture risk. Essential for long-term bone health monitoring.
CTS – Carpal Tunnel Syndrome: Compression of the median nerve at the wrist. Causes numbness, tingling, and hand weakness. Often treated with splints, injections, or surgery.
OA – Osteoarthritis: Degenerative joint disease due to cartilage breakdown. Causes pain, stiffness, and reduced range of motion. Common in hips, knees, and hands.
RSI – Repetitive Strain Injury: Overuse injury to muscles, tendons, or nerves. Common in wrists, elbows, and shoulders. Preventable with ergonomic adjustments.
Fractures & Fixation
FNF – Femoral Neck Fracture: Break in the neck of the femur, common in elderly after falls. High risk of complications due to disrupted blood supply. Treated with screws, arthroplasty, or hemiarthroplasty.
Fx / Frx – Fracture: Break in a bone. Classified by pattern, location, and stability. May require casting, fixation, or surgery.
DHS – Dynamic Hip Screw: Implant system for stabilizing femoral neck or intertrochanteric fractures. Allows controlled compression during healing. Inserted surgically into the femur.
SHS – Sliding Hip Screw: Similar to DHS, used for hip fracture stabilization. Provides controlled movement as the fracture heals. Widely used in orthopaedic trauma.
IMN – Intramedullary Nail: Rod placed inside bone marrow canal for fracture stabilization. Common in long bone fractures. Provides strong internal fixation.
CMN – Cephalomedullary Nail: Type of intramedullary nail extending into the femoral head. Stabilizes proximal femur fractures. Often chosen for unstable hip fractures.
ORIF – Open Reduction Internal Fixation: Surgical repair of fractures using plates, screws, or rods. “Open reduction” means exposing the bone surgically. “Internal fixation” stabilizes it from inside.
Ex-fix – External Fixator: Frame with pins/wires inserted into bone through skin. Stabilizes fractures or corrects deformities externally. Used in severe trauma or infection cases.
Arthroplasty & Joint Replacement
THA – Total Hip Arthroplasty: Complete hip replacement with artificial components. Relieves pain from arthritis or fractures. Improves mobility and quality of life.
TKA – Total Knee Arthroplasty: Replacement of the knee joint with artificial implants. Used for end-stage arthritis or deformity. Restores function and reduces pain.
TSA – Total Shoulder Arthroplasty: Replacement of the shoulder joint with prosthesis. Improves motion and relieves pain. Used for arthritis or severe fractures.
RSA – Reverse Shoulder Arthroplasty: Shoulder replacement where ball and socket are reversed. Provides stability when rotator cuff is deficient. Useful in complex shoulder conditions.
DFR – Distal Femoral Replacement: Prosthetic replacement of lower femur. Used in severe fractures or tumors. Restores knee joint stability and function.
Neuro & Physical Exam Terms
DTR – Deep Tendon Reflexes: Involuntary muscle contractions when tendon is tapped. Used to assess nerve and spinal cord function. Commonly tested in knees and ankles.
SILT – Sensation Intact to Light Touch: Exam finding documenting preserved skin sensation. Indicates intact nerve function. Common in trauma assessments.
AIN – Anterior Interosseous Nerve: Branch of the median nerve controlling thumb/index finger flexion. Injury causes weakness in pinch grip. Tested with “OK sign.”
PIN – Posterior Interosseous Nerve: Branch of the radial nerve controlling finger extension. Injury causes finger drop. Often injured in forearm trauma.
Motion & Weight Bearing
FROM – Full Range of Motion: Joint can move normally in all planes. Indicates absence of stiffness or contracture. Often documented in rehab notes.
PROM – Passive Range of Motion: Movement performed by examiner without patient effort. Tests joint flexibility and stiffness. Important in rehab and post-op recovery.
AROM – Active Range of Motion: Movement performed by patient voluntarily. Assesses muscle strength and function. Limited in cases of weakness or pain.
NWB – Non-Weight Bearing: Patient must not put weight on injured limb. Requires crutches, walker, or wheelchair. Standard after major fractures or surgery.
PWB – Partial Weight Bearing: Patient may put limited weight on limb. Usually specified as percentage (e.g., 25%). Step-down progression in rehab.
TTWB – Toe Touch Weight Bearing: Only toes lightly touch the ground for balance. No real weight through limb. Transition stage before partial weight bearing.
FFWB – Foot Flat Weight Bearing: Patient may rest entire foot but not load limb. Intermediate between TTWB and PWB. Used for gradual progression.
WBAT – Weight Bearing as Tolerated: Patient bears as much weight as comfortable. Limited only by pain. Common after stable fracture fixation.
Trauma & Mechanism
APC – Anterior Posterior Compression: Pelvic fracture pattern from front-to-back force. Causes pelvic instability and bleeding risk. Often from high-energy trauma.
LC – Lateral Compression: Pelvic fracture pattern from side-to-side force. Stability varies with severity. Common in vehicle or crush injuries.
GLF – Ground-Level Fall: Fall from standing height. Common cause of hip and wrist fractures in elderly. Often signals osteoporosis or frailty.
GSW – Gunshot Wound: Penetrating trauma from firearm. May involve bone, nerves, and vessels. Requires multidisciplinary care.
Materials
Provider & Professional Acronyms
Physicians
MD – Doctor of Medicine: Completed allopathic medical training. Focuses on traditional biomedical model. Trained in surgery, prescribing, and full scope practice.
DO – Doctor of Osteopathic Medicine: Completes same training as MD with additional focus on holistic care and musculoskeletal system. Uses osteopathic manipulative treatment (OMT). Licensed for full practice in the U.S.
Additional Physician Types
PA-C – Physician Assistant, Certified: Graduate-level medical provider trained in diagnosis, treatment, and minor surgery. Works under physician supervision. Can prescribe medication.
NP – Nurse Practitioner: Advanced practice registered nurse with graduate-level training. Provides diagnosis, treatment, and prescribing. Often emphasizes preventive and holistic care.
DNP – Doctor of Nursing Practice: Highest clinical degree for nursing. Focuses on leadership, evidence-based practice, and advanced clinical skills. Functions as an NP with expanded academic training.
Nursing & Allied Health
RN – Registered Nurse: Provides patient care, medication administration, and coordination. Licensed after nursing degree and national exam. Backbone of hospital and surgical teams.
LPN – Licensed Practical Nurse: Provides basic patient care under RN supervision. Training shorter than RN. Common in rehab and outpatient settings.
CNA – Certified Nursing Assistant: Assists patients with daily living tasks. Works under nurses’ supervision. Provides vital bedside support.
CRNA – Certified Registered Nurse Anesthetist: Advanced practice nurse specializing in anesthesia. Provides anesthesia independently or with anesthesiologists. Critical in surgery and trauma care.
Therapy & Rehabilitation
PT – Physical Therapist: Doctorate-level provider specializing in mobility, strength, and rehab. Designs exercise programs for recovery. Critical after surgery or injury.
DPT – Doctor of Physical Therapy: Doctoral degree in physical therapy (entry-level in U.S.). Focuses on evidence-based rehab care. Equivalent to PT but emphasizes doctoral training.
OT – Occupational Therapist: Helps patients regain independence in daily activities. Focuses on upper extremity function and adaptive strategies. Important post-surgery or after injury.
COTA – Certified Occupational Therapy Assistant: Works under OT supervision. Delivers therapy exercises and training. Provides hands-on patient support.
ATC – Athletic Trainer, Certified: Specializes in sports medicine, injury prevention, and rehab. Works with athletes and orthopaedic teams. Provides on-field and clinical support.
Surgical & Training Roles
FA – First Assistant: Assists primary surgeon with exposure, suturing, and technical tasks. Can be physician, PA, or NP. Enhances operative efficiency.
SA – Surgical Assistant: Supports surgeon intraoperatively with retraction, suction, and prep. May be trained staff or non-physician. Distinct from scrub nurse.
PGY-# – Post-Graduate Year: Indicates level of residency training. Example: PGY-3 = third-year resident. Determines experience and role in surgery.
MS4 – Fourth-Year Medical Student: Final year before graduation from medical school. May assist in surgery under supervision. Limited responsibilities compared to residents.
Certifications
FAAOS – Fellow of the American Academy of Orthopaedic Surgeons: Prestigious membership after board certification in orthopaedics. Indicates commitment to education and peer standards. Recognized globally in orthopaedics.
FACS – Fellow of the American College of Surgeons: Designation for surgeons meeting rigorous professional standards. Shows commitment to ethical and skilled surgical practice. Used across multiple specialties.
Understanding Tylenol, Advil, and Aleve: A Parent’s Guide
A Quick Note: When it comes to over-the-counter medicine, we highly encourage you to talk to your doctor about what you are using or plan to use. It's not a good idea to take advice about medicine on the internet without consulting a medical professional. The information here is designed to give you a great overview of the differences, the main effects, and why or how they work. This is not intended to replace actual medical advice!
When your child has pain or a fever, it’s common to reach for over-the-counter medicine. But which one is best—Tylenol, Advil, or Aleve? Each works differently in the body, has different age guidelines, and comes with important safety points. This guide walks you through what each option does, how long it lasts, and when it may be appropriate so you can make the safest choice.
Key Differences at a Glance
Brand
Active Ingredient
Category
Main Effects
Tylenol
Acetaminophen
Analgesic / Antipyretic
Reduces pain and fever, but not inflammation
Advil / Motrin
Ibuprofen
NSAID
Reduces pain, fever, and inflammation
Aleve
Naproxen
NSAID
Reduces pain, fever, and inflammation; lasts longer per dose
Both Advil and Aleve are NSAIDs, which are especially helpful when swelling is part of the problem. Tylenol is not an NSAID, but it’s effective for lowering fever and easing pain without affecting inflammation.
Age Guidelines and Surgery Considerations
Tylenol can be used in infants (consult a doctor for recommended dose), and in most cases it may be given up until the time of surgery unless your surgeon advises otherwise.
Advil is not recommended for children younger than 6 months. Families should follow their surgeon’s guidance on timing before surgery—many ask families to stop ibuprofen about 3 days beforehand, but instructions can vary.
Aleve (OTC naproxen) isn’t recommended for children under 12 unless a clinician specifically advises it. Prescription naproxen may sometimes be used for pediatric conditions under physician supervision.
Safety Tips Every Parent Should Follow
Always measure carefully. Use the provided cup, dropper, or syringe. Kitchen spoons are not accurate.
Check every label. Many cold or flu medicines already include acetaminophen or an NSAID. Doubling up can cause harm.
Keep a log. Writing down the time of each dose helps prevent giving medicine too soon.
Consider health conditions. If your child has liver disease, consult their clinician before giving acetaminophen; it’s contraindicated in severe or active liver disease. Children with kidney or stomach issues may need to avoid NSAIDs.
Stay hydrated. Ibuprofen and naproxen are not recommended if your child is dehydrated because of the risk to the kidneys.
Store medicines safely. Keep them in original containers, out of reach, with caps closed tightly.
Which One Should You Choose?
If your child has swelling from an injury, an NSAID like Advil or Aleve may help. If you’re treating pain or fever without swelling, Tylenol is often a safe choice. Some families alternate Tylenol with an NSAID to avoid exceeding safe limits for either drug, but this should only be done under your doctor’s guidance.
When to See an Orthopaedic Specialist
Pain lasts for more than a few days or keeps returning.
You notice swelling, warmth, or stiffness in a joint.
Your child avoids using the limb or can’t put weight on it.
Over-the-counter medicine doesn’t improve symptoms.
Our team can help you understand what’s behind the pain, make safe choices about medicines, and design a plan that includes activity, rest, and recovery strategies.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
What Can Help Relieve Herniated or Bulging Disc Pain?
A common back and spine problem is herniated or bulging discs. Nearly everyone will know someone who has experienced a herniated disc at some point in their lives. It's painful and we hope you're one of the fortunate ones who don't have to endure it. In many cases, these discs will heal on their own with no long-term consequences. However, if you have a herniated disc and aren’t able to treat it successfully by yourself, you may need to reach out for professional help from an experienced physical therapist or orthopaedist.
Fortunately, there are several exercises that can ease the pain caused by a herniated disc and strengthen your back to prevent relapses.
Core stabilization exercises
Many people suffering from back pain have weak core muscles. When the core muscles are weak, the spine receives less support. This may be a reason why people with weak core muscles experience back pain more often than those who have a strong core. Core stabilization exercises strengthen the core and make your body less prone to back pain. One of the best exercises to strengthen the core is the pelvic tilts. It should be done in two variants to strengthen your core in different ways. Another exercise that strengthens your core is the bent knee hug. Other exercises that strengthen the core are the bicycle and the knee to chest. Other core stabilization exercises you can try are:
Planks
Side plank
floor prone cobra
cable anti-rotation (requires equipment found at most gyms.)
Stretching Exercises
A herniated or bulging disc can lead to muscle spasms in your back. Thus, it’s recommended that you stretch your muscles as often as possible to ease the pain and prevent muscle spasms from becoming chronic. There are many great stretches that you can do to ease the back pain caused by a herniated disc.
The knee to chest is one of the best stretches that you can do on a daily basis. It will help you ease the pain caused by a herniated disc and improve your overall posture. To perform this stretch, you should lie on your back and use your hands to grab one leg by the ankle. Next, you should pull that leg towards your chest and hold this position for 30 seconds. After performing this stretch, you should repeat it with the other leg. This is one of the best knee-to-chest stretches that you can do while dealing with a herniated disc. It will help you ease the pain caused by the condition and improve your overall posture. These are the best exercises that you can do while dealing with a herniated disc. They will help you ease the pain caused by the condition and also improve your posture.
One of the best stretches is the hip stretch. It will help you ease the pain in your back and improve the blood flow to your lower extremities. To perform this exercise, you should lie on the floor and use your arms to pull one leg up towards your head. Next, you should try to reach your hands towards your toes while keeping the other leg on the floor.
Another great stretch is the triceps stretch. You should perform this stretch while standing upright. Then, you should lift one arm towards the sky while keeping the other arm on your side. You should hold this position for about 30 seconds and then perform the same stretch with the other arm. This stretch will help you ease the pain caused by a herniated disc and improve your overall posture.
Finally, the seated hamstring stretch. It will help you ease the pain in the back of your leg and improve your posture. To perform this exercise, you should sit on a chair and place one leg on another. Then, you should try to bend towards the leg that’s on the chair. You should perform this stretch for 30 seconds and then switch legs. These are the best stretching exercises that you can do while dealing with a herniated disc. They will help you ease the pain caused by the condition and also improve your posture.
Exercises To Avoid With A Herniated Disk
Not all stretching and exercises are created equal, especially when it comes to herniated and bulging disc pain. A lot of folks experience this pain when bending and rotating their body. This ought to tell you that rotational exercises aren't the ones you want to try out. Leg raises are also out since they tend to put a lot of stress on the lower back. You should also avoid sit-ups and a common runner's stretch - toe touches. These will often exacerbate the pain and potentially do more damage to the injured disc.
Other Solutions For A Herniated Disk
Of course, gentle stretching and exercising may not be the solution to your herniated or bulging disc problem. Before trying any of these stretches or exercises, you should consult with one of our spine and neck specialists to make sure that you're not doing something which could contribute to future damage. We can begin with physical therapy which may get rid of the issue altogether. If that doesn't work, there are other options including surgery. Your case will be unique so no matter what we encourage you to set up an appointment with us today.