Exercises to Relieve Lower Back Pain: A Step-by-Step Guide
Lower back pain is common, and the right movements can make a big difference. This guide walks you through simple mobility drills, gentle stretches, and core-strengthening exercises, plus how often to do them, how to stay safe, and when to see a specialist at Princeton Orthopaedic Associates.
What You'll Learn
How to move your back safely without flaring symptoms.
Mobility exercises that ease stiffness.
Core and hip strengthening that supports your spine.
Stretching for tight hips, hamstrings, and glutes.
A simple weekly routine you can follow.
What to do if pain increases during a movement.
Signs you should pause and contact a clinician.
How often to practice and how to progress safely.
Ways our team can personalize your plan.
When imaging or further evaluation may be appropriate.
Before You Start: Safety, Setup, and Pain Rules
These movements should feel gentle and controlled. You may notice a comfortable stretch or mild muscular effort, but you should not experience sharp, stabbing, or worsening pain at any point during the exercise. If you feel uncomfortable, ease back, rest briefly, and check your form. Move slowly, keep your movements smooth, and breathe steadily throughout each position.
Warm-up: 3 to 5 minutes of easy walking or marching in place.
Breathing: Inhale through your nose, exhale through pursed lips.
Avoid holding your breath during exercises.
Range of motion: Stay in a pain-free range and ease in gradually.
Surface: Use a yoga mat or carpet for comfort.
Stop if you notice new numbness, leg weakness, or pain traveling below the knee that intensifies.
Mobility First: Gentle Movements to Reduce Stiffness
Begin with slow, comfortable movements to ease the back and improve blood flow throughout the spine. Move with control, staying in a pain-free range, and stop if anything sharp or increasingly uncomfortable appears. For most moves, aim for about five to ten deliberate repetitions unless otherwise noted.
1) Pelvic Tilts (Supine)
Lie on your back with knees bent and feet hip-width apart.
Gently flatten your low back toward the floor by tightening your abdominals, then return to neutral.
Perform 1 to 2 sets of 8 to 12 reps.
2) Lower Trunk Rotations
On your back with knees bent, slowly roll both knees to one side, pause, then roll to the other side.
Keep shoulders relaxed against the floor.
5 to 10 reps each side.
3) Single Knee to Chest
Bring one knee toward your chest using your hands or a towel behind the thigh.
Hold 15 to 30 seconds, switch sides.
Repeat 2 to 3 times per side.
4) Cat to Cow
On hands and knees, gently round your spine up, then lengthen it as you look slightly forward.
Move slowly with your breath.
8 to 10 slow reps.
5) Child’s Pose Reach
Sit back toward your heels with knees comfortable, reach arms forward, and relax your torso.
Hold 20 to 30 seconds, 2 to 3 times, staying pain-free.
Build Support: Core and Hip Strengthening
Strong hips and a steady core help unload irritated tissues in the lower back and support your spine during daily tasks. Perform each movement with deliberate control, paying attention to alignment and how your body feels. If any symptom worsens, stop the exercise and reassess your form. Aim for two to three sets, with 30 to 60 seconds of rest between sets.
1) Bridge
On your back, knees bent, feet planted.
Squeeze glutes and lift hips until shoulders, hips, and knees form a line.
Pause 2 seconds, lower slowly; 8 to 12 reps.
2) Bird Dog
From hands and knees, brace your core.
Extend opposite arm and leg without arching your back.
Hold 2 to 3 seconds; 6 to 10 reps per side.
3) Dead Bug (Modified)
On your back, hips and knees bent to about 90 degrees, arms up.
Keep your low back gently anchored to the floor.
Tap one heel to the floor and return; switch sides; 6 to 10 reps per side.
4) Side-Lying Clamshell
Lying on your side with knees bent, keep feet together.
Lift the top knee without rolling your hips; 10 to 15 reps per side.
5) Forearm Plank (Knees or Toes)
Maintain a long spine, keep ribs and pelvis aligned.
Hold 10 to 20 seconds without pain; 2 to 4 holds.
Stretch What's Tight: Hips and Legs
Tight hips or hamstrings can pull on the pelvis and increase back strain. Hold each stretch 15 to 30 seconds, repeat 2 to 3 times, and keep breathing.
Hamstring Strap Stretch: On your back, loop a strap or towel around the foot and gently straighten the knee until a mild stretch is felt in the back of the thigh.
Hip Flexor Stretch: Half-kneeling, gently shift your weight forward until you feel the front of the hip stretch on the kneeling side.
Piriformis Figure-4: Cross one ankle over the opposite knee and draw the legs toward your chest until the outer hip stretches.
A Simple Weekly Plan
Use this plan as a flexible starting point and adjust it based on how you feel and what you can tolerate. Prioritizing consistency and gradual progress matters more than pushing for fast gains. Listen to your body, and modify days, reps, or rest as needed to stay comfortable and avoid flare-ups.
Day
Mobility
Strength
Stretch
Notes
Mon
Pelvic tilts, trunk rotations
Bridge, clamshell
Hamstrings
Easy start, 1 to 2 sets
Tue
Cat to cow
Bird dog
Hip flexors
Focus on form
Wed
Child’s pose
Dead bug
Piriformis
Optional walk 10 to 20 min
Thu
Pelvic tilts, trunk rotations
Bridge, clamshell
Hamstrings
Add 1 to 2 reps if comfortable
Fri
Cat to cow
Bird dog
Hip flexors
Short and easy
Sat
Choice mobility
Plank holds
Piriformis
Walk or light activity
Sun
Recovery
—
Gentle stretch
Listen to your body
Progress Tips
Increase reps or holds by small amounts once a week if movements feel easy and symptoms stay settled.
Keep motions smooth and controlled, not fast or jerky.
Add short daily walks to support circulation and recovery.
Use supportive footwear and avoid prolonged sitting when possible.
When to Pause and Contact a Clinician
Most back pain improves with gentle activity and careful pacing, but some warning signs require medical input sooner rather than later. If your symptoms persist beyond a short period, intensify, or there are new concerns, seek medical guidance promptly. The list below describes red flags that warrant evaluation by a clinician.
Severe or worsening pain that doesn’t change with rest.
Leg numbness, tingling, or weakness that’s increasing.
Changes in bowel or bladder control.
Fever, unexplained weight loss, or recent significant trauma.
How Princeton Orthopaedic Associates Can Help
If your symptoms aren’t improving, our team can evaluate your movement, identify the source of pain, and build a program that fits your goals. Most people do well with focused physical therapy, activity modification, and a progressive home plan.
If you’re unsure where to start, schedule an exam with our spine or physical therapy team. We’ll help you understand what’s safe, how to progress, and when additional options are appropriate.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
Elbow Tendinopathy: What It Is and How We Treat It at Princeton Orthopaedic Associates
Elbow tendinopathy is a common overuse injury that causes pain and tenderness in the tendons around the elbow. It happens when these tendons—connecting muscle to bone—become irritated from repeated stress. In this blog, you’ll find simple home treatments that can help relieve symptoms and learn when it’s time to see a specialist.
Quick overview
We’ll cover what causes elbow tendinopathy, the differences between lateral and medial types, practical home care tips, rehab strategies like strengthening and stretching, and when injections or surgery might be needed.
What Is Elbow Tendinopathy?
Elbow tendinopathy is an overuse condition where the tendons around your elbow become irritated. Tendons connect muscles to bone, and when they’re overloaded they can be painful and tender.
There are two common forms. Lateral elbow tendinopathy affects the outer elbow and is often called tennis elbow. Medial elbow tendinopathy affects the inner elbow and is often called golfer's elbow. Both share similar causes and treatments.
What Causes Elbow Tendinopathy?
Repeated or forceful wrist and arm motions are the usual culprits. These motions create small tears and inflammation in the tendon where it attaches to the bone.
Repeated gripping or twisting of the wrist
Working with vibrating tools or heavy lifting
Poor technique in sports or tasks that load the forearm
Weakness in the wrist or shoulder that shifts stress to the elbow
Simple Steps You Can Try at Home
Many people feel better with early conservative care. Try these measures for several weeks while monitoring symptoms.
Modify activities that cause pain and avoid repetitive motions when possible
Ice the area for 10 to 15 minutes every few hours to reduce pain and swelling
Use over the counter anti inflammatory medication if it’s safe for you and your doctor agrees
Wear a counterforce strap or supportive brace during aggravating activities
Rehabilitation: Exercises and Therapy
Physical therapy is the mainstay for lasting relief. A therapist will show you targeted exercises to rebuild tendon health and correct movement patterns.
Eccentric strengthening of the wrist extensor or flexor muscles helps rebuild tendon tolerance
Grip strengthening and progressive loading programs are used once pain improves
Stretching and manual therapy help reduce tightness in the forearm and shoulder
Other Medical Treatments
If symptoms persist despite conservative care, your provider may discuss additional options. These are considered after a careful evaluation.
Corticosteroid injections may offer short term relief in select cases, but guidelines warn about potential tendon weakening or rupture with repeated use. A careful, shared decision process helps decide if this option fits your goals and activity level [AAOS guidelines 2020; NICE guidelines 2021].
PRP injections, a type of biologic treatment, may be discussed when appropriate. Current evidence is mixed and appears to depend on the specific tendinopathy and stage of injury; decisions should be individualized based on patient needs [Cochrane review on PRP for tendinopathy 2019; AAOS guidelines 2020].
Surgery is rarely needed and is reserved for persistent tendon damage that affects function
Recovery Timeline
Recovery varies with how long symptoms have been present and how consistently you follow rehab recommendations.
Therapy and strengthening restore function for most people
Chronic
2 months or longer
May need advanced treatments and extended rehab for full recovery
Preventing Recurrence
Once your pain improves, keep working on strength, flexibility, and technique. Those steps reduce the chance that tendinopathy will come back.
Practice ergonomic changes at work and during activities
Use proper form for sports and lifting
Build balanced strength in the forearm, shoulder, and core
Gradually increase activity load rather than jumping back in too fast
When You Should See Us
Contact our team if pain lasts despite home care, limits your daily tasks, or if you’re losing strength. We’ll evaluate your elbow, identify the root cause, and recommend a personalized plan.
Schedule an exam with one of our sports medicine doctors or physical therapists to get targeted treatment and a clear recovery plan.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
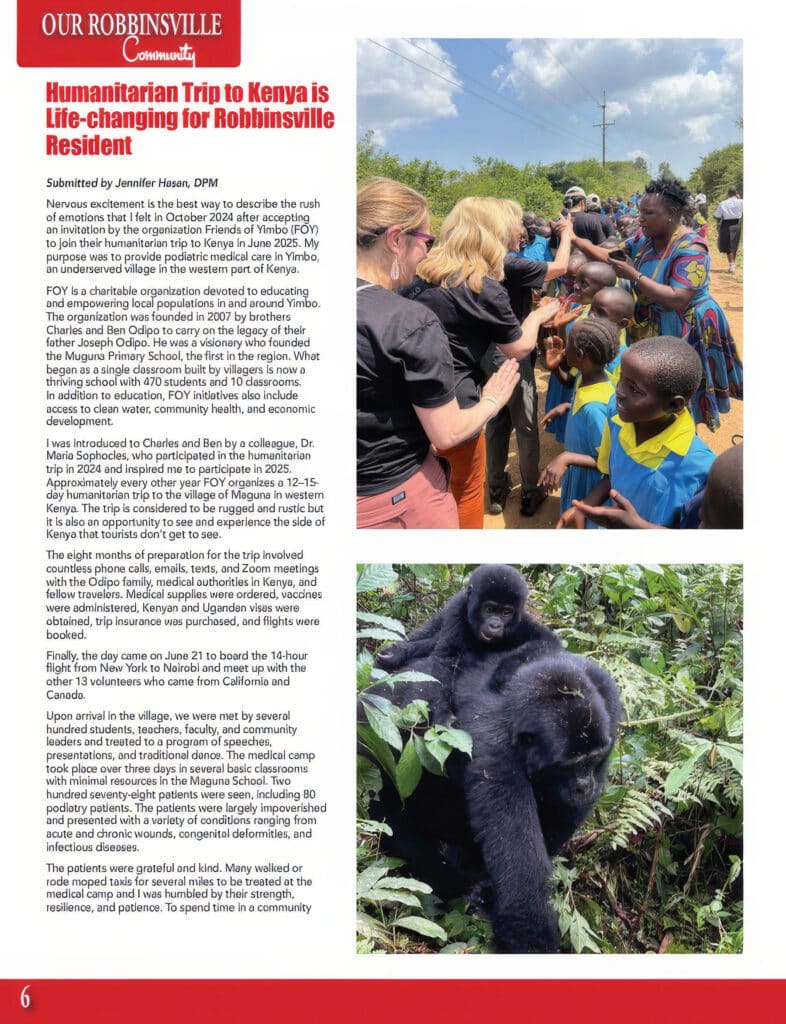
Friends of Yimbo (FOY)Bwindi Impenetrable Forest Jennifer Hasan, DPM
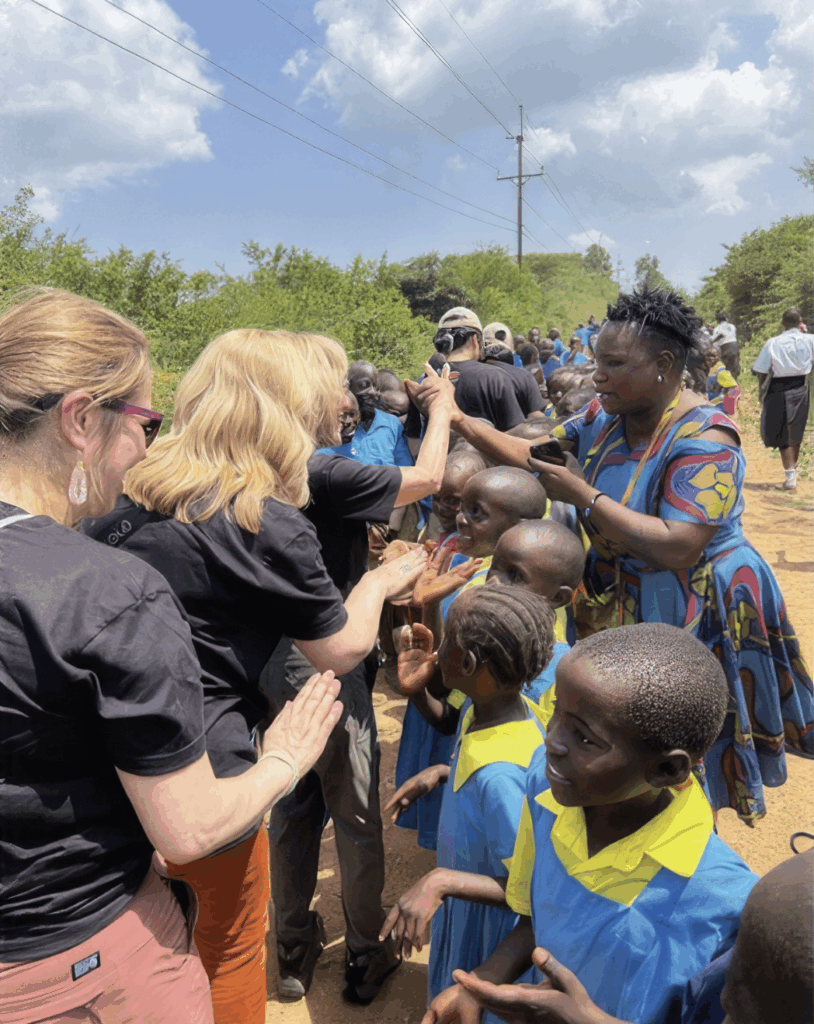
Humanitarian Trip to Kenya is Life-changing for Robbinsville Resident
Submitted by Jennifer Hasan, DPM
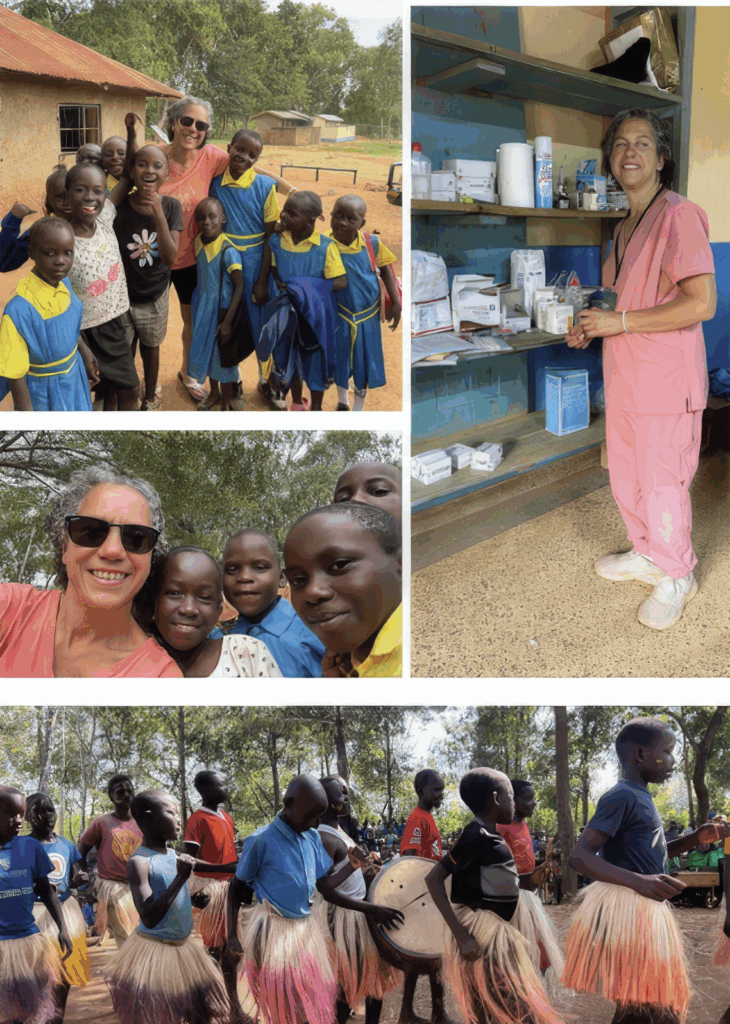
Nervous excitement is the best way to describe the rush of emotions that I felt in October 2024 after accepting an invitation by the organization Friends of Yimbo (FOY) to join their humanitarian trip to Kenya in June 2025. My purpose was to provide podiatric medical care in Yimbo, an underserved village in the western part of Kenya.
FOY is a charitable organization devoted to educating and empowering populations in and around Yimbo. The organization was founded in 2007 by brothers Charles and Ben Odipo to carry on the legacy of their father Joseph Odipo. He was a visionary who founded the Muguna Primary School, the first in the region. What began as a single classroom built by villagers is now a thriving school with 470 students and 10 classrooms. In addition to education, FOY initiatives also include access to clean water, community health, and economic development.
I was introduced to Charles and Ben by a colleague, Dr. Maria Sopchede, who participated in the humanitarian trip in 2024 and inspired me to participate in 2025. Approximately every other year FOY organizes a 12–15-day humanitarian trip to the village of Muguna in western Kenya. The trip is considered to be rugged and rustic but it is also an opportunity to see and experience the side of Kenya that tourists don’t get to see.
The eight months of preparation for the trip involved countless phone calls, emails, texts, and Zoom meetings with the Odipo family, medical authorities in Kenya, and the travelers. Medical supplies were ordered, vaccines were administered, Kenyan and Ugandan visas were obtained, trip insurance was purchased, and flights were booked.
Finally, the day came on June 21 to board the 14-hour flight from New York to Nairobi and meet up with the other 13 volunteers who came from California and Canada.
Upon arrival in the village, we were met by several hundred students, teachers, faculty, and community members and treated to a program of speeches, presentations, and traditional dance. The medical camp took place over three days in several basic classrooms within small enclosures in the Muguna School. Two hundred seventy-eight patients were seen, including 80 podiatry patients. The patients were largely impoverished and presented with a variety of conditions ranging from acute and chronic wounds, congenital deformities, and infectious diseases.
The patients were gentle and kind. Many walked or rode moped taxis for several miles to be treated at the medical camp and I was humbled by their strength, resilience, and patience. To spend time in a community where most live on less than a dollar a day and lack basic necessities such as electricity and running water and yet are proud, resourceful, and happy offers a new perspective of one’s own life and challenges.
After five days in Yimbo our group split up to visit other destinations in Africa including Mount Kilimanjaro in Tanzania, Madagascar, and Uganda. I joined seven others for a once-in-a-lifetime experience in the Bwindi Impenetrable Forest in southwestern Uganda to see mountain gorillas in their natural habitat. After an eight-hour drive from Kampala we navigated through rugged terrain accompanied by a guide, trackers, security guards and porters to observe these gentle and majestic animals for one hour. Standing three feet away from a 400 lb. silverback gorilla was awe-inspiring moment that I will never forget.
The finale of the trip was a safari in the Masai Mara National Reserve in southwestern Kenya known for its high concentration of wildlife including the “Big Five” (lion, leopard, elephant, buffalo, and rhino). We saw all except the elusive leopard. We were also able to experience the Great Migration of wildebeests and zebras from Tanzania into Kenya which begins in July.
In the end, this was so much more than a humanitarian trip. The bonds of friendship made within the Friends of Yimbo and with my fellow travelers will last a lifetime. It was an honor and a privilege to experience the warmth and hospitality of the villagers who trusted me with their medical care. I would encourage others to come out of their comfort zone for this type of experience—and who knows…you just may see a leopard!
Dr. Jennifer Hasan has resided in Robbinsville for 15 years with her husband Kevin Greczek, and teenage sons Jacob and Adam Greczek. She is the Chief of Podiatry at Penn Medicine Princeton Medical Center. She has practiced podiatric medicine and surgery at Princeton Orthopaedic Associates for 22 years.
She would like to thank Dr. Maria Sophocles for introducing her to FOY and Princeton Orthopaedic Associates for their generous contribution of medical supplies for this mission.
Page 1Page 2
Improve Your Posture: Simple Steps You Can Start Today
Good posture means your head, shoulders, and hips line up with your spine. This helps your body work well and move with less pain. Small, steady changes can add up over days and weeks. This guide explains why posture matters, common reasons it slips, safe exercises, and quick ergonomic setup ideas you can use at home or work to feel better and move more easily.
Good posture helps distribute forces evenly across your joints and muscles. When posture is poor, some muscles take on extra work while other areas weaken, which can lead to neck, shoulder, or back pain. The encouraging part is that steady, small changes usually lead to meaningful improvements.
What This Guide Covers
What healthy posture looks like and why it matters.
Common causes of posture problems.
Easy daily habits, stretches, and strengthening moves.
Simple ergonomic changes for home and office.
When to seek clinical care.
What is Good Posture?
Good posture means your head, shoulders, and hips line up so your spine is supported and muscles can work efficiently. It doesn’t mean you must sit perfectly rigid. Instead, aim for balance: a neutral spine with relaxed shoulders and an engaged core.
When your posture is balanced, less stress sits on joints and soft tissues, and you’re less likely to develop pain from overuse or compensatory movement patterns.
Why Posture Matters for Everyday Comfort
Posture affects pain, breathing, and how you move. Slouching can make neck and upper back muscles work harder. It can also change how your shoulders and hips move, which may lead to recent or gradual pain.
Poor posture can increase neck, shoulder, and lower back strain
It can reduce your tolerance for standing or walking for long periods
Correcting posture helps with balance and reduces the chance of developing compensatory injuries
Common Reasons Posture Slips
Sitting for long stretches without breaks
Weakness in the mid-back, glutes, or core muscles
Tight chest or hip flexor muscles
Poor workstation setup or unsupportive shoes
Holding one-sided positions, like carrying a heavy bag on one shoulder
Daily Habits You Can Start Today
Set a timer to stand and move every 30 minutes
When sitting, keep your feet flat, hips level, and shoulders relaxed
Use a rolled towel or lumbar roll for lower back support if needed
Switch which hand you use for tasks that are one-sided, such as carrying groceries
Simple Stretches and Strengthening Moves
These choices are low-risk and can be done at home. Start gently and increase repetitions over weeks as you feel stronger. Evidence from major guidelines supports regular practice, with adults typically performing strengthening 2 to 3 days per week and stretches held for 20 to 30 seconds, gradually increasing as tolerated. (ACSM guidelines 2023)
Chin tucks: Slide your head back, keeping eyes forward to strengthen deep neck muscles. Do 8 to 12 reps. Safety: keep a neutral neck and avoid tucking the chin so far you feel pain or strain. If you have neck pain, numbness, or tingling, stop and consult a clinician. Frequency: 2–3 days per week.
Thoracic extensions: Sit upright and gently arch the mid-back over a chair back to improve upper spine mobility. Repeat 8 to 10 times. Safety: maintain a tall spine, do not strain the neck, and stop if you feel joint pain. Frequency: 2–3 days per week.
Glute bridges: Lie on your back, press hips up while squeezing glutes to build hip support. Do 10 to 15 reps. Safety: keep the spine in a neutral line, press through the heels, and stop if you feel sharp back pain. Frequency: 2–3 days per week.
Wall angels: Stand with your back to a wall and slide arms up and down to open the chest and strengthen the mid-back. Do 8 to 12 reps. Safety: keep head, shoulders, and butt against the wall; avoid arching the lower back. Frequency: 2–3 days per week.
Hip flexor stretch: Kneel on one knee and push hips forward to stretch the front of the hip. Hold 20 to 30 seconds each side. Safety: keep the pelvis level, avoid overarching the lower back, and stop if you feel pain. Frequency: 2–3 days per week.
Ergonomic Fixes That Help
Position your monitor at eye level to support a neutral spine and an ergonomic setup
Use a chair that supports the curve of your lower back
Keep frequently used items within easy reach
Try a sit-stand routine if you work at a desk
Choose shoes with good support for standing jobs
What Progress Looks Like and How Long It Takes
People improve at different speeds. Small changes can show up in a few weeks if you practice regularly. Bigger, longer standing posture problems take longer to improve and may need a tailored plan. A steady mix of simple strengthening moves, daily posture habits, and help from a clinician or physical therapist can help you move better and reduce pain.
Issue
Typical time to notice change
Notes
Minor slouching
2 6 weeks
Daily breaks and basic exercises usually help.
Moderate postural imbalance
4 6 weeks
Requires consistent strengthening and ergonomic changes.
Long-standing posture-related pain
2+ months
Often needs a tailored program from a clinician or physical therapist.
When You Should See a Clinician
Try the self-care tips for a week or two. See a specialist sooner if pain limits your daily activities, if you change how you walk or move to avoid pain, or if home measures don’t help.
Provider
What they help with
Primary care or sports medicine
Initial evaluation and recommendations for non-surgical care
Physical therapist
Hands-on treatment, personalized exercise programs, posture training
Physiatrist
Complex movement problems, chronic pain management, coordinate care
At Princeton Orthopaedic Associates, we assess the root cause of posture problems and work with you to build a practical plan. We focus on restoring function and helping you return to activities with less pain.
Getting Started: An Easy Plan
Set small goals: three short sessions per day of targeted exercises
Add movement breaks: stand and walk for a few minutes each half hour
Adjust your workspace: monitor height, seat support, and footwear
Track progress: note changes in comfort and ability to do daily tasks
If you need help customizing a program or you have persistent pain, schedule an exam so we can evaluate you and design a specific plan.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
Gout: Symptoms, Risks, Testing, and Treatment
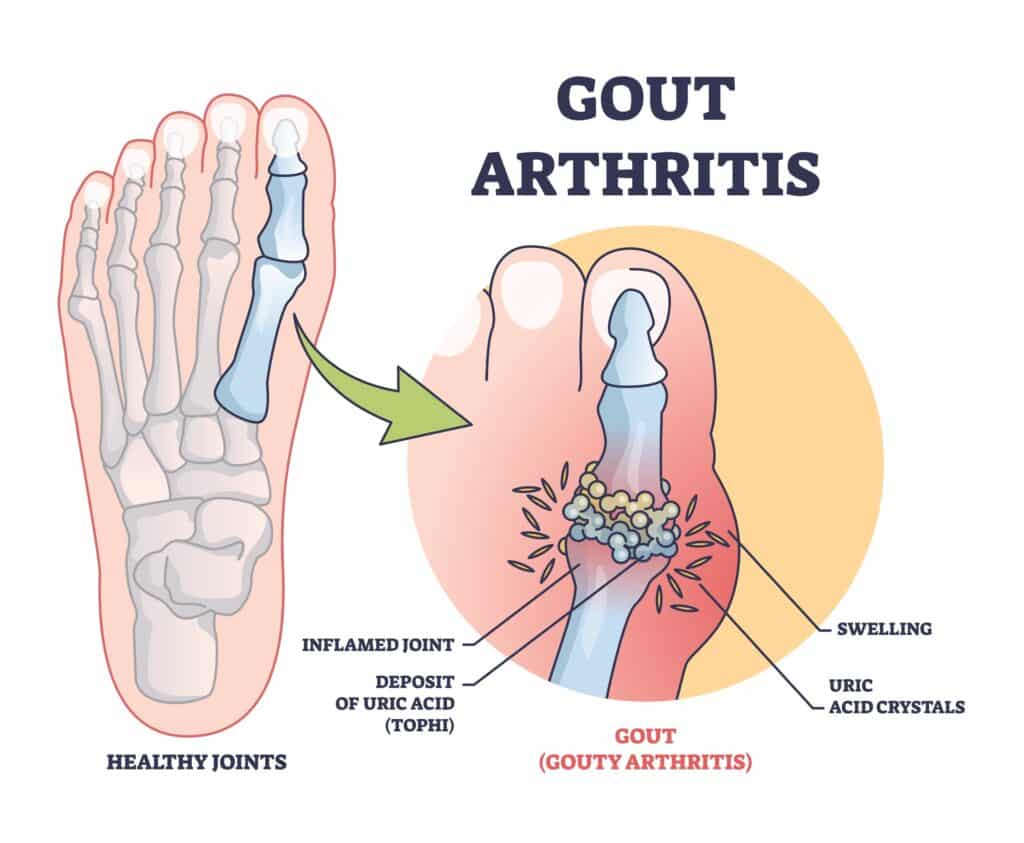
Gout is a common type of inflammatory arthritis that causes sudden, intense joint pain and swelling. In this guide, you will learn what gout is, why it happens, who is at higher risk, how we diagnose it, and the treatments that help you feel better and prevent future flares.
What Is Gout?
Gout happens when uric acid builds up in the blood and forms needle-like crystals inside a joint. Your immune system reacts to those crystals, which triggers sudden pain, redness, heat, and swelling. The big toe is the classic spot, but gout can affect the midfoot, ankle, knee, wrist, fingers, and elbow.
How Gout Feels
Sudden, severe pain that often starts at night.
Redness, warmth, and swelling at one joint.
Extreme tenderness where even a bedsheet can hurt.
Stiffness and limited motion during and after a flare.
With long-standing gout, firm bumps under the skin called tophi can develop.
Why Gout Happens
Uric acid forms when your body breaks down purines, which are found naturally in your tissues and in certain foods. When production is high or your kidneys don’t clear enough uric acid, crystals can deposit in joints and surrounding tissues. Cold areas like the big toe are common sites for crystal formation.
Who Is at Higher Risk?
Age and sex: more common in men and after menopause in women
Family history of gout or high uric acid
Chronic kidney disease or reduced kidney function
Metabolic conditions: obesity, insulin resistance, high blood pressure, high triglycerides
Medications: diuretics for blood pressure, low-dose aspirin, cyclosporine, tacrolimus
Dietary factors: frequent alcohol use, especially beer and spirits, red and organ meats, certain seafoods like anchovies and shellfish, and sugar-sweetened beverages with fructose
When to Seek Care
If you notice a new hot, swollen joint or have repeated gout flares, seek care promptly from a clinician or urgent care provider. Early evaluation helps confirm that gout is the cause, guides fast pain relief, prevents infection or other problems, and protects the joint from lasting damage. A clinician will review your health history and medicines to choose safe, effective treatment and avoid drug interactions.
Severe joint pain with redness and warmth
Fever or feeling unwell along with a hot, swollen joint can signal a joint infection (septic arthritis). Seek urgent same-day medical evaluation to rule out infection before receiving steroid injections or NSAID-only treatment.
Recurrent attacks in the same or different joints
Hard nodules near joints or the ear rim that may be tophi
How We Diagnose Gout
During your visit, a clinician will look at the painful joint and review your overall health, symptoms, and medicines. The best way to confirm gout is to take a tiny sample of joint fluid and check it under a microscope for uric acid crystals. This test helps rule out infection and other problems that can look like gout.
Joint aspiration and crystal analysis when possible
Blood tests, including uric acid level, kidney function, and markers of inflammation
Imaging when needed: ultrasound can show a double contour sign, X-rays reveal long-term changes, and specialized CT may identify crystal deposits
Treating an Acute Gout Flare
Flares respond best when treatment starts early. The main goal is to ease pain quickly, reduce swelling, and lower inflammation while protecting the affected joint from more harm. Your doctor will tailor medicines to your health history and current medicines to ensure safety and effectiveness and help you return to daily activities.
Anti-inflammatory medicines such as NSAIDs, if safe for you
Colchicine, especially when started soon after symptoms begin
Corticosteroids by mouth or a targeted joint injection
Rest, elevation, and ice for comfort
Do not stop your long-term urate-lowering medicine during a flare unless your doctor advises it. Let us know at the first sign of a flare so we can tailor treatment to your health history and medications.
Preventing Future Attacks
If you have repeated flares, tophi, kidney stones from uric acid, or moderate to advanced chronic kidney disease, you may benefit from urate-lowering therapy. The aim is to keep your blood uric acid below target so crystals dissolve and flares fade over time.
Topic
Key Points
Who Should Start Urate-Lowering Therapy
2 or more flares per year, tophi, uric acid kidney stones, or chronic kidney disease stage 3 or higher
First-Line Medicine
Allopurinol is typically first choice. Start low and increase gradually. Febuxostat is another option if needed. In patients with established cardiovascular disease, febuxostat carries an FDA boxed warning for increased risk of cardiovascular death. Use only after shared decision-making, and consider allopurinol first. Allopurinol can rarely cause severe cutaneous adverse reactions. Consider HLA-B*58:01 testing in high-risk groups (e.g., Han Chinese, Thai, Korean patients with CKD, and African American patients) before starting therapy.
Other Options
Probenecid may help if kidney function is adequate. Pegloticase is reserved for severe, refractory cases. Less effective with moderate-to-severe CKD; avoid or use cautiously in patients with a history of uric acid kidney stones; review for drug–drug interactions.
Target Uric Acid
Under 6 mg/dL is the usual goal. Under 5 mg/dL may be used if tophi are present.
Flare Prevention When Starting Therapy
Low-dose colchicine or an NSAID is often used for several months to reduce flare risk during dose adjustments.
Daily Steps That Help
Maintain a healthy weight and stay active within comfort
Limit alcohol, especially beer and spirits
Moderate high-purine foods like red and organ meats and certain seafoods
Cut back on sugar-sweetened drinks, especially those with fructose
Drink water regularly and review medications with your doctor
Possible Complications If Gout Is Not Treated
Tophi that can erode bone and limit joint motion
Progressive joint damage and arthritis
Uric acid kidney stones
How Princeton Orthopaedic Associates Can Help
Our team evaluates the painful joint, confirms the diagnosis, and builds a treatment plan that eases pain fast and prevents future attacks. When appropriate, we can perform joint aspiration or an image-guided injection and coordinate long-term urate-lowering therapy with your broader care team.
If you think you're having a gout flare or you've had recurrent attacks, schedule an evaluation. Getting ahead of flares now helps protect your joints for the long term.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
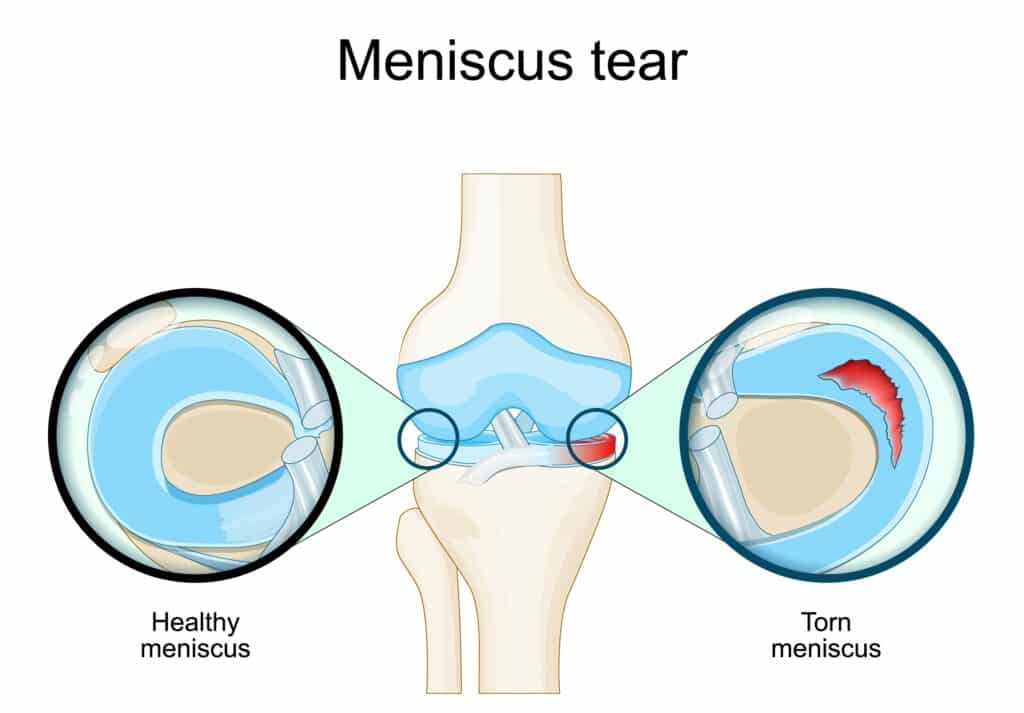
Torn Meniscus: What It Is, How It Happens, and How We Treat It
Understand what a meniscus tear is, the symptoms to watch for, how it’s diagnosed, and available treatment options. Learn when it’s best to see a specialist and what recovery typically involves so you can make informed decisions about your knee health.
A torn meniscus is a common knee injury that affects the cartilage pads that cushion your thigh bone and shin bone. You may get one from twisting your knee during sports or from gradual wear as you get older. Symptoms and treatments vary, and we walk through what you can expect at each step.
Quick Facts You Should Know
Your menisci are C shaped cartilage pads that help absorb shock and stabilize the knee.
Tears can occur suddenly with a twist or develop slowly from degeneration.
Common symptoms include pain, swelling, catching or locking, and difficulty fully straightening the knee.
Treatment ranges from rest and physical therapy to arthroscopic surgery depending on the tear and your goals.
Young people often have traumatic tears from sports.
Older adults may have degenerative tears that happen with everyday activities.
Some tears can heal with nonoperative care; others need repair or trimming.
We focus on restoring function so you can return to the activities you enjoy.
The menisci are rubbery wedges of cartilage that sit between your femur and tibia. They help spread load across the knee joint, absorb shock, and add stability when you twist or change direction.
When a meniscus tears, the knee loses some of that cushioning. That can cause pain with activity, swelling, and catching sensations. Over time, untreated problems can change how the joint wears, which may increase the risk of arthritis for some people.
What a Meniscus Tear May Feel Like
Pain along the joint line, often on the inside or outside of the knee.
Swelling that can appear right away or develop over 24 to 48 hours.
A catching, locking, or a sense that the knee gives way.
Tenderness when pressing along the joint line.
Limited ability to fully straighten the knee.
Pain that increases with twisting or squatting motions.
Common Ways Meniscus Tears Occur
Tears usually come from one of two patterns. Younger people often tear their meniscus during a forceful twist, pivot, or tackle. Older adults may develop a tear from gradual wear as the cartilage weakens with age.
Traumatic injury during sports or a fall.
Twisting the knee while the foot is planted.
Degenerative changes that make the meniscus fragile over time.
Repetitive squatting or kneeling that stresses the cartilage.
How We Diagnose a Meniscus Tear
We start with a focused history and knee exam. Certain exam maneuvers help us identify likely meniscal problems, and we check for swelling, range of motion, and mechanical symptoms.
If we need to confirm the diagnosis or plan treatment, imaging such as MRI is often helpful because it shows soft tissue details. X rays can rule out arthritis or bone issues.
Treatment Options: What to Expect
Treatment depends on your symptoms, the tear type and location, your age, and your activity goals. We focus on relieving pain, restoring function, and protecting long term joint health.
Nonoperative Care
Rest, ice, compression, and elevation to control pain and swelling.
Anti inflammatory medication if appropriate and recommended by your provider.
Physical therapy to strengthen muscles around the knee and improve movement patterns.
Activity modification to avoid motions that make symptoms worse while you recover.
Procedures and Surgery
If symptoms persist or there is a mechanical block in the knee, we may recommend arthroscopic surgery. Two common approaches are meniscal repair and partial meniscectomy.
Meniscal repair aims to sew the torn pieces back together when healing potential is good. It preserves meniscus tissue and helps protect the joint long term.
Partial meniscectomy trims the damaged portion when repair is not possible. This often reduces symptoms quickly but removes some cushioning.
Typical Recovery Timelines
Recovery varies based on the treatment chosen and the tear itself. Below are common timelines to help set expectations.
Treatment
Usual Recovery
Notes
Conservative care
Several weeks to a few months
Many people improve with therapy and activity changes.
Partial meniscectomy
4 to 8 weeks for many daily activities
Return to sports may be faster but depends on rehab and surgeon guidance.
Meniscal repair
3 to 6 months
Requires protected rehab to allow healing of the repaired tissue.
When You Should See a Specialist
If your knee locks or you can not fully straighten it.
If swelling or pain does not improve with a few weeks of rest and therapy.
If you have persistent instability or can not return to your normal activities.
Who to see at Princeton Orthopaedic Associates
Specialty
When to Choose
Role
Sports Medicine
Acute injuries and nonoperative care
Diagnosis, rehab planning, and nonsurgical management
Orthopedic Surgeon (Knee)
Persistent symptoms or mechanical problems
Discuss surgical options and perform arthroscopy when needed
Physical Therapy
Recovery after injury or surgery
Hands on care and guided strengthening to restore function
Simple Steps to Reduce Your Risk
Keep leg muscles strong, especially your quadriceps and hamstrings.
Practice balance and agility drills to reduce awkward twists.
Use proper footwear and replace shoes when they wear out.
Warm up before activity and avoid sudden increases in activity level.
If you want help protecting your knee or recovering from a meniscus tear, schedule an exam with one of our specialists. We personalize care so you can get back to your life with confidence.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
Understanding and Managing Hand Cramps
Quick overview
Hand cramps are sudden, involuntary squeezes of the muscles in your hand or fingers. They can happen during activity or at rest and often respond to simple measures, but sometimes they point to an underlying issue that needs professional care.
What Are Hand Cramps?
A hand cramp is a tight, often painful contraction of one or more hand muscles that you cannot relax immediately. They usually happen without warning and can last from a few seconds to several minutes.
Squeezing or knotting feeling in the palm or fingers
Difficulty opening the hand while the muscle is tight
Sometimes a visible twitch or hard lump under the skin
Common Triggers for Hand Cramps
Several everyday factors can make hand cramps more likely. Often more than one factor is involved.
Muscle overuse from repetitive tasks like typing, sewing, or gripping tools
Muscle fatigue after unusual or prolonged hand activity
Dehydration or mineral imbalances such as potassium, magnesium, or calcium can contribute in some contexts, but not all cramps require supplementation
Nerve irritation or compression in the wrist or forearm
Certain medications or medical conditions that affect nerves or muscles
What a Hand Cramp Feels Like
Hand cramps can vary from a mild tightness to a painful spasm. They may affect one finger, several fingers, or the whole hand. Symptoms often come on suddenly and can interfere with normal hand use until the muscle relaxes.
Sharp or aching pain during the spasm
Stiffness or reduced grip strength afterwards
Occasional tingling if a nerve is involved
Immediate Steps to Ease a Cramp
If a cramp starts, try these simple measures to help the muscle relax. These steps are safe for most people and often work quickly.
Stop the activity that triggered it and gently stretch the affected finger or hand
Massage the tight muscle using light pressure to increase blood flow
Apply a warm compress if the muscle feels tight, or cold if there is sharp pain after activity
Drink water; if dehydration or electrolyte imbalance is suspected, seek clinician guidance and appropriate testing; routine potassium or magnesium supplementation for isolated hand cramps is not universally recommended
Try shaking your hand or opening and closing the fingers slowly to help the spasm pass
Note: If cramps happen frequently, or are severe, it is important to get a medical review to find the cause.
Longer Term Strategies to Prevent Recurrence
Preventing hand cramps often means addressing how you use your hands and caring for overall muscle and nerve health. Small daily changes can reduce episodes significantly.
Take regular short breaks during repetitive tasks to rest and stretch
Use ergonomic tools and adjust your workspace to reduce strain on the wrist and hand
Strengthen hand and forearm muscles with guided exercises if recommended by a therapist
Stay hydrated and eat a balanced diet that includes minerals important for muscle function
Consider splinting at night if cramps wake you from sleep or if a nerve problem is suspected
When to See a Doctor
See a clinician if cramps are persistent, frequent, worsening, occur at rest without clear triggers, or are accompanied by numbness and weakness. Those signs may indicate a nerve or systemic issue that needs evaluation.
Who Can Help
Specialist
When to Choose
Notes
Primary Care Provider
First evaluation, blood tests, medication review
Good starting point to rule out common causes
Orthopaedic Hand Specialist
Suspected structural or nerve problems in the hand or wrist
Helps correct movement patterns and build hand endurance
Neurologist
Frequent cramps with weakness or other neurological signs
Assesses nerve disorders and coordination
Treatment Options Your Specialist May Discuss
Treatment depends on the cause. Many people improve with conservative measures. In select cases, targeted therapies may be recommended.
Activity modification and ergonomic changes
Guided hand and forearm exercise programs with a therapist
Medication review and correction of electrolyte or metabolic issues
Botulinum toxin injections are not standard for routine hand cramps. They are generally considered only in rare focal dystonias or specific nerve related conditions, and carry risks such as focal weakness
Simple Hand Stretches You Can Try
These gentle stretches may reduce tightness and build resilience. Stop if they cause sharp pain and check with a clinician if you have an injury.
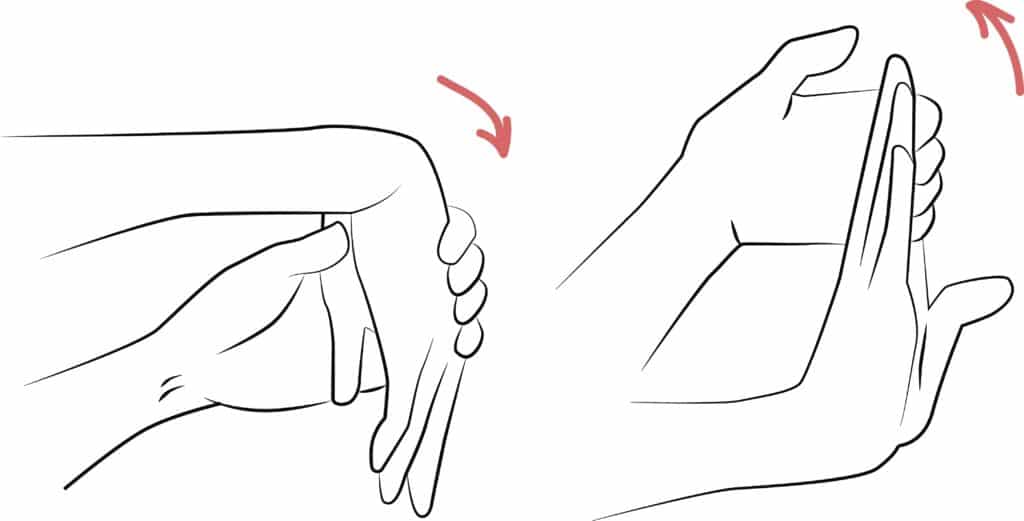
Finger extension: gently bend the fingers back with the other hand and hold for 15 to 30 seconds
Thumb stretch: pull the thumb away from the palm and hold for 15 seconds
Wrist flexor stretch: straighten the arm, bend the wrist down with the palm facing out, and hold
How Long Until I Feel Better?
Recovery varies by cause and how soon you begin appropriate care. Many people improve within days when the issue is temporary. If cramps come from nerve compression or a chronic condition, recovery may take weeks to months with therapy and targeted treatment.
Typical Pattern
Timeframe
What Helps
Acute, activity related
Days to weeks
Rest, hydration, stretching
Recurrent with overuse
Several weeks
Ergonomic changes, therapy
Nerve-related (peripheral nerve compression) or other nerve-related causes
Weeks to months
Specialist evaluation and targeted care
Living With Occasional Hand Cramps
Most people can manage occasional cramps with simple self-care and small changes to daily routines. If cramps limit your work or hobbies, we can help find the right plan so you can stay active and comfortable.
If your cramps are persistent or troubling, schedule an exam with one of our hand specialists. We will review your history, examine your hand, and recommend tests or therapy if needed. Together we will create a plan tailored to your needs.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
Why Does My Knee Pop? Common Causes and When to Get Help
Learn why knees sometimes pop, when it’s usually harmless, and when it may signal a problem. Common causes include gas bubbles or tendons snapping, but popping can also point to joint issues. Explore simple at-home steps that may help, and know when it’s time to see a clinician.
If you hear occasional popping without pain, it is usually not serious. But if popping comes with pain, swelling, instability, or locking, you should seek evaluation so we can find the cause and plan treatment.
Quick Overview: What This Post Covers
What makes knees pop.
How to tell harmless popping from trouble.
Simple self-care and when to see a specialist.
Tests and treatments your clinician may use.
How we approach diagnosis and recovery at Princeton Orthopaedic Associates.
Common, Usually Harmless Causes of Knee Popping
Sometimes popping is simply noise from normal joint movement. A few common benign reasons include:
Gas bubbles forming and popping inside the joint fluid, which can create a cracking sound
Tendons or ligaments snapping briefly as they shift over bone when the joint moves
Rough surfaces rubbing in a joint with age-related wear; osteoarthritis can also have inflammatory flares and management depends on symptoms and function
Painless popping alone is not known to cause arthritis; however, if popping is accompanied by pain, swelling, instability, or limits on function, you should have it evaluated.
When Popping May Mean a Problem
Popping that comes with other symptoms may point to an underlying injury. Watch for these signs:
Sharp or persistent pain at the time of popping
Visible swelling or the knee feeling hot
A feeling that the knee gives way, locks, or will not fully bend or straighten
Pain or instability that limits walking or daily activities
Those symptoms suggest we should examine the joint to look for cartilage injuries, meniscal tears, ligament strain, loose fragments, or significant joint inflammation.
Emergency or Urgent Signs
If any of the following occur after a pop, get urgent or emergency care rather than waiting for a routine appointment:
A loud pop during an injury followed by immediate swelling and inability to bear weight
Visible deformity or suspected patellar dislocation
The knee is locked and you cannot fully straighten it - true mechanical locking
Severe pain after trauma or when a fracture is suspected
A hot, very painful swollen knee with fever or chills, or a swollen painful knee in someone who is immunocompromised - possible septic arthritis
What Might Be Causing Painful Popping?
Several common issues can cause painful popping. These include damage to soft tissues, cartilage problems, and mechanical irritation around the joint.
Meniscal tears. A torn meniscus can catch or lock and may produce a pop with pain.
Ligament sprains. A sudden twist or direct blow can cause ligament stretching and an audible pop.
Patellar tracking issues and patellar instability or dislocation. If the kneecap moves unevenly or subluxes, you may feel or hear snapping and experience pain.
Loose bodies or osteochondral injury. Cartilage or bone fragments can catch in the joint and cause painful popping or locking.
Cartilage wear. As cartilage thins with age or injury, joint surfaces can make noise and become painful.
How We Evaluate Popping Knees
Your clinician will take a careful history and perform a focused exam to check motion, stability, and areas of tenderness. That helps narrow down likely causes.
Imaging and tests are selected based on the history and exam. X-rays are often first-line after trauma to assess for fracture and alignment; X-rays do not show soft tissues. MRI is ordered when the exam or history suggest soft tissue injury such as meniscus or ligament tears, cartilage damage, or when mechanical symptoms persist. Ultrasound can be useful for dynamic snapping and for evaluating superficial tendon or bursal problems.
Test
What it shows
X-ray
Bone alignment, fracture, and evidence of arthritis; does not show soft tissues
MRI
Soft tissues like meniscus, ligaments, and cartilage; used when exam or history suggest soft tissue injury or persistent mechanical symptoms
Ultrasound
Tendon or bursa irritation near the knee and useful for dynamic snapping
At-home Steps You Can Try First
If popping is mild and not accompanied by the concerning signs above, try conservative care while watching symptoms. Small changes often help.
Rest from the activity that triggers the sound for a few days
Ice the area for 10 to 15 minutes if there is pain or swelling
Over-the-counter nonsteroidal anti-inflammatory drugs may reduce pain; avoid NSAIDs if you have a history of gastrointestinal ulcers or bleeding, kidney disease, are taking blood thinners, are in late pregnancy, or have an NSAID allergy. If NSAIDs are not appropriate, consider acetaminophen after checking with your provider
Start gentle strengthening and mobility work for hips, quads, and hamstrings; a physical therapist can guide this
When You Should Schedule an Exam
Contact us for an evaluation if you have persistent pain, swelling, catching or locking, repeated giving way, or if symptoms prevent daily tasks. Early assessment helps us treat the cause and reduce the chance of longer term issues.
Who to See at Princeton Orthopaedic Associates
Specialty
Why you would see them
Sports Medicine
Non surgical evaluation for tendon, ligament, and meniscal problems
Orthopaedic Surgeon
Persistent mechanical symptoms or when surgery may be needed
Physical Therapist
Rehabilitation to improve strength, control, and movement patterns
What to Expect from Treatment
Treatment depends on the diagnosis. Many causes improve with a planned rehab program that reduces pain, restores motion, and strengthens supporting muscles. When structural damage is severe, surgical options may be discussed.
Conservative care first: activity modification, medication, targeted therapy
Procedures: injections may help for persistent inflammation
Surgery: reserved for clear mechanical problems or unresolving structural injury
If you want to discuss symptoms, we make it easy to schedule an exam. A focused visit helps us determine what is normal and what needs treatment so you can get back to your routine with confidence.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
That Aching or Sharp Pain in Your Shin Might Be Shin Splints
Whether you’re just trying to stay active, chasing after your kids, or if it's your teen pushing through practices and games, shin splints can stop you in your tracks. That aching, sometimes sharp pain along the front of the leg isn’t only for athletes running marathons, it’s surprisingly common in everyday life. Kids in fall sports like soccer, football, and cross-country often run into it, but parents and adults who spend long hours on their feet or squeeze in workouts can feel it too. What starts as a dull soreness after activity can quickly turn into a daily frustration, making simple things like walking, climbing stairs, or enjoying playtime harder than they should be. Shin splints don’t just interrupt sports; they interrupt life. This post explains what causes shin splints, how they feel, how we diagnose them, and practical steps you can take to feel better. We cover common triggers, home care, when to see a specialist, and what recovery usually looks like.
What this article will help you understand
You’ll learn why shin splints happen, what symptoms to watch for, which everyday habits make them worse, and how we at Princeton Orthopaedic Associates approach treatment and recovery.
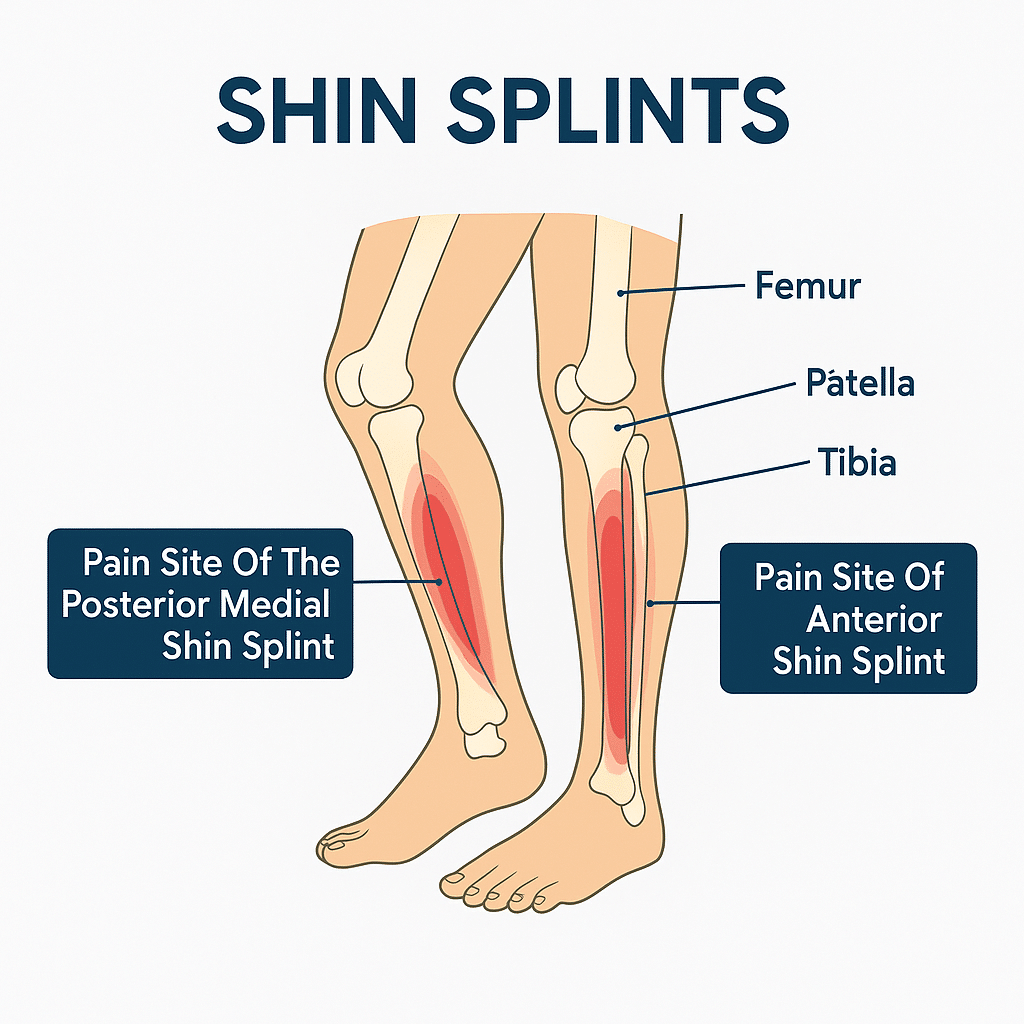
What Are Shin Splints?
Shin splints is a common name for pain along the shin bone that starts with activity. Classic shin splints most commonly refer to medial tibial stress syndrome, or MTSS, which presents as a diffuse aching along the posteromedial, or inner, border of the lower tibia near the distal half of the shin. Persistent pain over the front of the shin is less typical for MTSS and may indicate a tibial stress fracture or exertional compartment syndrome, so those symptoms should be evaluated.
MTSS is not just simple surface inflammation. It sits on a bone stress continuum where repeated overload affects the tibial cortex and the periosteum, and traction from muscles such as the soleus and tibialis posterior contributes to symptoms. We keep explanations simple but want you to know the pain often reflects mechanical overload of bone and the tissues attached to it.
How Shin Splints Typically Feel
Symptoms of shin splints usually start as a dull, aching pain along the inner edge of the lower leg, often felt during activity and easing with rest early on. The pain typically covers a broader segment along the posteromedial tibia rather than a single sharp spot.
Tenderness when you press along the shin, usually over a longer segment along the inner border
A dull, aching pain during or after exercise that may improve with rest at first
Visible swelling is uncommon in shin splints; marked swelling should prompt evaluation for other causes
Pain that gets worse if activity continues without change
By contrast, a tibial stress fracture more often causes focal point tenderness, a small spot that is exquisitely painful to press. Exertional compartment syndrome may produce tightness, cramping, numbness, or weakness during activity. If your pain is sharp, highly localized, wakes you at night, or makes it hard to walk, see a clinician promptly to check for these possibilities.
Common Causes and Who’s at Risk
Shin splints come from repetitive stress on the lower leg. You don’t have to be a runner to get them; they happen with many forms of exercise and work that increase load on the shin.
Sudden increases in training distance, speed, or duration
Starting a new activity without gradually building up
Running on hard or uneven surfaces
Worn or unsupportive shoes
Flat feet, high arches, or poor foot mechanics
Tight calf muscles or weak muscles that stabilize the ankle and foot
How We Confirm the Diagnosis
Diagnosis starts with a careful history and a physical exam. We check the pattern of pain, how it changes with activity, and look at your foot and ankle mechanics. The exam helps distinguish shin splints from a focal stress fracture or from exertional compartment syndrome.
If needed, imaging can help rule out a stress fracture or other conditions when symptoms are severe, very focal, or not improving with appropriate rest. X-rays are often the first test but can be normal early on. If concern persists, an MRI is more sensitive and can confirm a bone stress injury.
Treatment You Can Start at Home
Rest from the activity that worsens pain until symptoms improve
Ice the painful area for 15 to 20 minutes several times a day
Use over-the-counter pain relievers only as your clinician recommends. If a stress fracture is suspected, for example if you have night or rest pain, focal bony tenderness, or pain with hopping, avoid NSAIDs and consider acetaminophen until you are evaluated
Try low-impact cross-training like swimming or cycling while you recover
Gently stretching tight calves and working on ankle mobility can help. Do not push through sharp pain during exercises. If symptoms suggest a stress fracture or compartment syndrome, stop the aggravating activity and seek evaluation.
Hands-on Care and Rehab
If symptoms persist, physical therapy is often the next step. A therapist will guide you through strengthening and flexibility work to correct the forces that stress the shin and help you return to activity safely.
Strengthening exercises for the calves, foot muscles, and hips
Progressive return-to-activity plans to avoid re-injury
Gait and footwear assessment, orthotics when appropriate
How Long Recovery Usually Takes
Recovery time varies based on severity and how quickly you address the cause. The table below gives a general idea.
Severity
Typical Recovery
Notes
Mild
2 to 4 weeks
Relative rest, icing, and gradual return usually helps.
Moderate
4 to 8 weeks
Often needs formal rehab and footwear changes.
Severe or Persistent
8 weeks or more
May require imaging and a structured rehab plan to avoid stress fracture risk.
Tips to Prevent Shin Pain from Returning
Increase training load slowly, by no more than 10 percent per week
Choose supportive shoes and replace them when they wear out
Add strength work for calves, hips, and foot muscles
Mix in low-impact cross-training to reduce repetitive stress
Run on softer surfaces when possible and avoid sudden downhill training
When You Should See a Provider
Seek care if pain is severe, gets worse despite rest, or you cannot put weight on the leg. Also see a clinician if pain wakes you at night, if you have marked swelling, or if you have new numbness or weakness.
Be alert for signs that need prompt or urgent evaluation, including:
Severe pain or inability to bear weight
Night pain or pain at rest that does not improve
Focal bony tenderness that is very painful to press, or pain with hopping, which may suggest a stress fracture
Escalating tightness in the lower leg during or after activity, new numbness or tingling, increasing weakness, foot drop, or pain that is out of proportion to the findings and does not settle with rest, which could indicate compartment syndrome
Worsening symptoms despite rest and conservative care
When foot mechanics, orthotics, or surgical options are considered
Helpful if foot structure contributes to repeat problems
Getting Back to Activity Safely
Return to activity should be gradual and guided by pain. Increase load slowly and stop if symptoms flare. A simple progression to consider is pain-free walking, then a pain-free single-leg hop, then light jogging. If those steps are comfortable, gradually increase duration and intensity while continuing strengthening and mobility work.
If you are unsure whether your pain is caused by shin splints or something more serious, schedule an exam so we can check you and recommend the right next steps.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
Pain On the Outside of Your Knee Could be IT Band Syndrome.
You don’t have to be a marathon runner to feel that nagging ache on the outside of your knee. The important thing? It might not actually be your knee. It might be a tight IT band, and unlike joint injuries, it requires a different kind of treatment focused on mobility and muscle balance.
Maybe it starts during your daily walk, or when you’re going up stairs. Perhaps it flares up when you get up from your desk or out of the car. It might even wake you up at night, pulsing in your outer thigh or hip, making it impossible to get comfortable. It doesn’t feel like an injury yet, the pain keeps coming back.
If this sounds familiar, there’s a good chance your iliotibial band (IT band) is involved. And the condition you might be dealing with is called IT Band Syndrome, a common cause of outer knee and hip pain that affects far more than just athletes.
Let’s walk through what’s happening in your body, why it hurts, and most importantly, what you can do to start feeling better.
Here Are The Things You Need to Know About IT Band Syndrome
What You Should Know:
Pain on the outside of your knee or thigh is a common sign of IT Band Syndrome, and it's not just a runner's problem.
You don’t have to be an athlete. Everyday movement, prolonged sitting, or climbing stairs can all trigger symptoms.
The pain is caused by tightness and friction where the IT band rubs against bone near the knee.
Stretching the IT band itself won't solve the issue. Instead, focus on loosening surrounding muscles and improving strength.
Symptoms often show up with walking, going downstairs, or after long periods of inactivity.
The discomfort may travel up to your hip, outer thigh, or glute region, especially when lying on your side.
Causes often include weak glutes or core, poor posture, or worn-out shoes that don’t offer enough support.
Foam rolling can help, but you want to target the glutes, quads, and TFL, not directly on the IT band.
Recovery requires more than rest. Strengthening, mobility work, and correcting how you move are essential.
Seeing a physical therapist can help you address the root cause and get long-term relief.
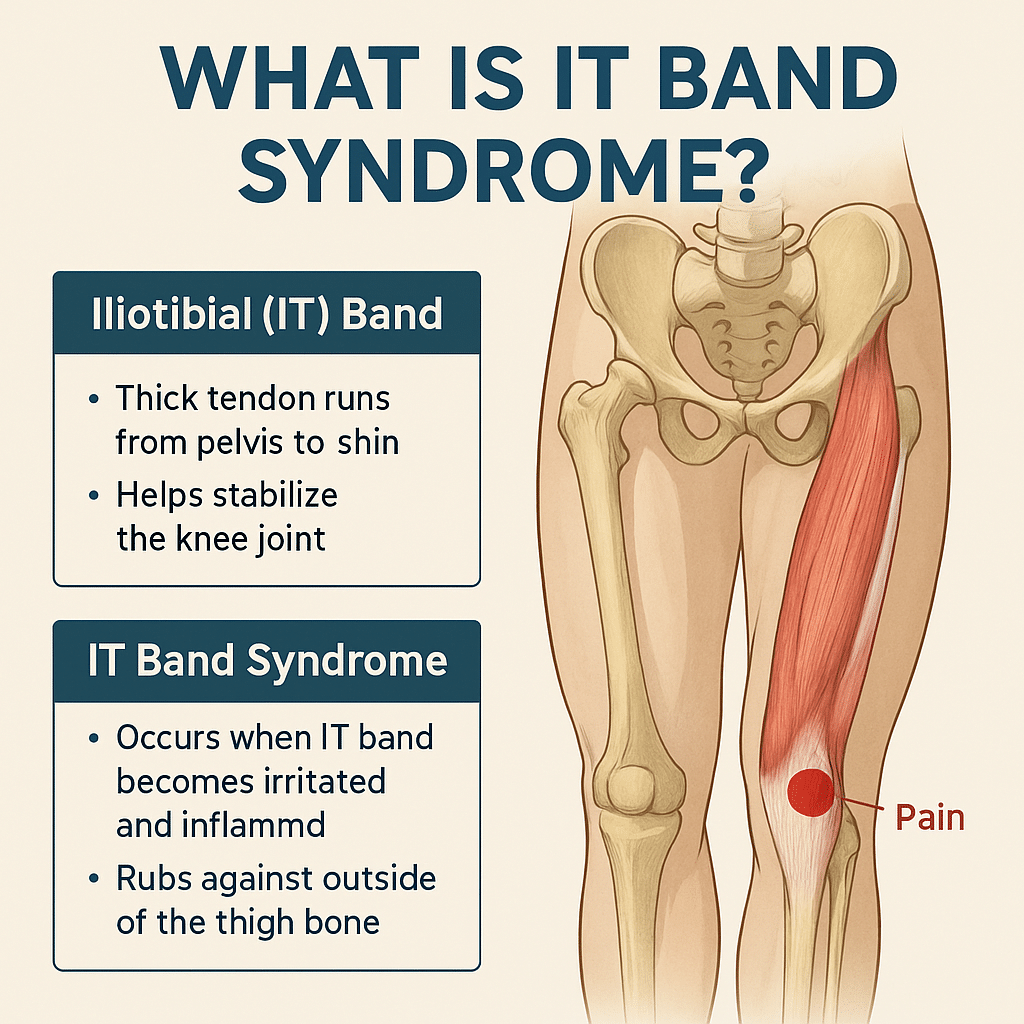
What Is the IT Band and Why Does It Get Tight?
The iliotibial (IT) band is a thick, fibrous band of connective tissue that runs down the outside of your leg, from your hip to just below your knee. Think of it as a support strap that helps stabilize your knee and assist with hip movement.
When the IT band gets too tight, often due to repetitive movement, muscle imbalances, or poor posture, it can rub against the bone at the outer knee. This creates irritation, inflammation, and pain, commonly known as IT Band Syndrome (ITBS).
And while it’s often associated with athletes, it’s just as common in walkers, desk workers, parents, nurses, retail workers, and anyone who’s on their feet a lot, or not enough.
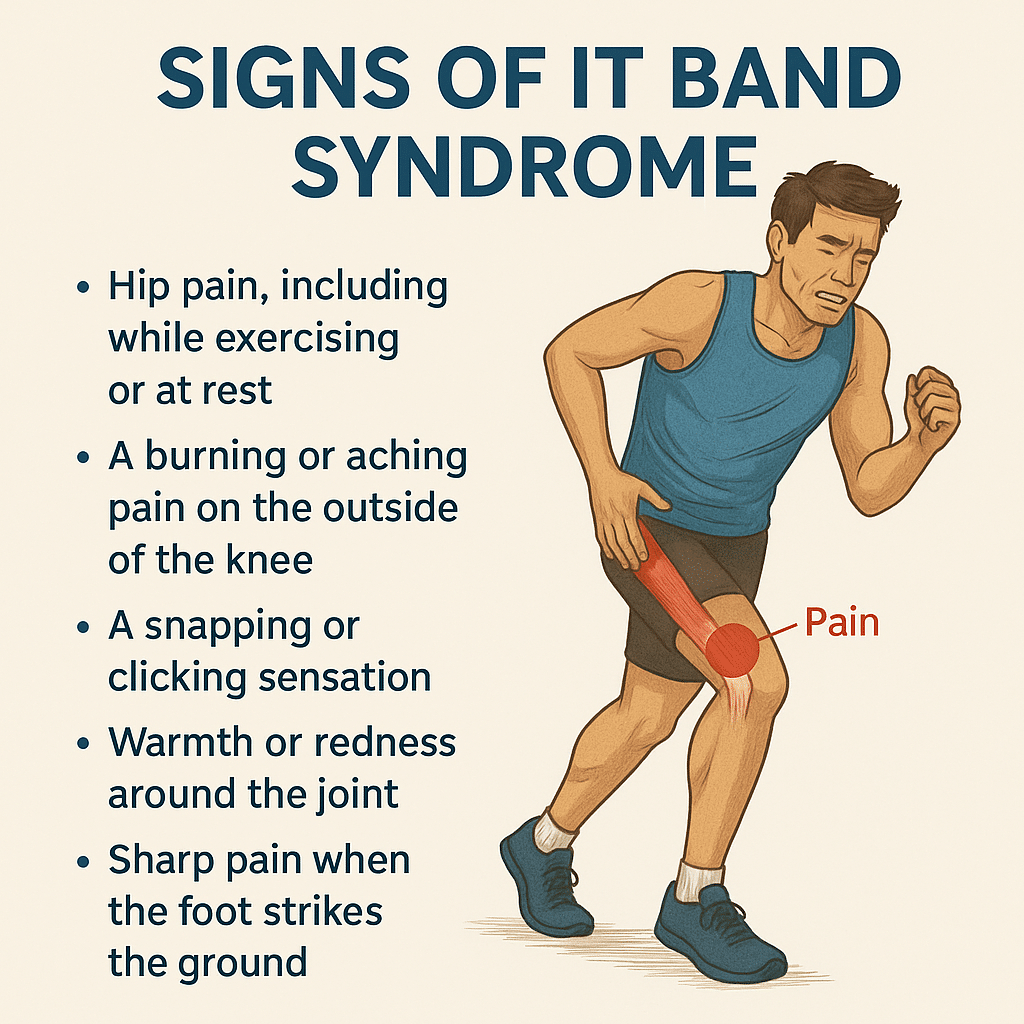
What Does IT Band Syndrome Feel Like?
Here are common, real-world symptoms of IT Band Syndrome in everyday life:
Aching or burning pain on the outside of the knee
Tightness or pulling in the outer thigh
Pain or discomfort going up or down stairs
Sharp pain with walking or standing for extended periods
Tenderness at the hip or discomfort when lying on your side
Clicking or snapping near the hip or knee
These symptoms often start mild, but become more consistent if left unaddressed.
What Causes IT Band Syndrome in Non-Athletes?
Even without intense training, everyday habits can contribute to ITBS:
Sitting for long periods without movement
Poor posture or weak hip/core muscles
Uneven walking surfaces (like sloped sidewalks or hilly neighborhoods)
Wearing worn-out or unsupportive shoes
Standing or walking with one leg favored over the other
Repetitive daily movement without adequate strength or flexibility
What Causes IT Band Syndrome in Athletes?
While the core problem is the same (tightness and friction along the IT band), athletes often develop ITBS due to training volume and biomechanics. Common athletic triggers include:
Sudden increases in mileage or intensity (especially in runners and cyclists)
Downhill running or running on sloped surfaces
Repetitive activities involving knee flexion and extension
Weakness in hip abductors, glutes, or core stabilizers
Poor running form or gait asymmetries
Worn shoes or improper footwear for training conditions
Overtraining without proper rest and recovery
IT Band Syndrome is common among:
Distance runners
Cyclists
Soccer and hockey players
HIIT or CrossFit athletes
Skiers or hikers tackling long descents
💡 Tip for athletes:
Strengthen your hips and glutes, cross-train, and make sure your recovery matches your training load
.
Why Is IT Band Pain So Persistent?
The IT band isn’t a muscle, it’s actually connective tissue. That means:
You can’t stretch it the same way you stretch a muscle
If surrounding muscles (like glutes and hip flexors) are tight or weak, the IT band picks up the slack
Without correcting imbalances, foam rolling or resting alone won’t fix it
Over time, the friction and inflammation can become chronic and much harder to treat.
How Is IT Band Syndrome Treated?
Treatment focuses on reducing inflammation, improving mobility, and correcting muscle imbalances.
✅ Pain Relief & Inflammation Control
Ice the outer knee or thigh for 15–20 minutes at a time
Use anti-inflammatory medication if recommended by your doctor
Strengthen glutes, hips, and core to support proper leg mechanics
Stretch hip flexors, quads, hamstrings, and TFL
Foam roll the surrounding muscle groups but not directly on the IT band
✅ Movement & Habit Adjustments
Improve running or lifting form through coaching or therapy
Modify walking and standing posture
Use ergonomic tools (e.g., standing desks, supportive chairs)
Wear supportive shoes or orthotics if needed
How Long Does IT Band Syndrome Take to Heal?
The length of time to recover from IT Band Syndrome depends on how long you've had symptoms and whether you're treating the root cause:
Severity
Recovery Time
Notes
Mild
2-3 Weeks
Rest and stretching may help quickly if caught early
Moderate
4-6 Weeks
Requires active rehab including movement correction
Chronic
2+ Months
Long-standing tightness or inflammation takes time to unwind
Everyday Life with IT Band Syndrome
IT Band Syndrome doesn't just show up during workouts; it can quietly interfere with our daily routine, mobility, and overall comfort. Without treatment, ITBS can impact your:
Ability to walk, climb stairs, or stand comfortably
Sleep (especially side-sleepers)
Workday (especially for those on their feet)
Confidence in movement and balance
Long-term joint health if compensatory patterns develop
And for athletes, it can put your training on pause or create a cycle of recurring injuries.
Should I See a Doctor for a Tight IT Band?
If you have been experiencing symptoms of IT Band Syndrome and you haven't found relief, you should consult with a specialist. Especially if:
The pain has lasted more than a week
You’ve tried rest but symptoms return
You’re changing how you move to avoid pain
You’re unable to stay active or complete daily tasks comfortably
At Princeton Orthopaedic Associates, we have physicians from multiple specialties that can help you get to the root of your tight IT band and help set you off on the path to recovery.
- A physical therapist is often the next step after diagnosis for hands-on treatment and long-term recovery.
Our specialists will identify the root cause of your tightness, guide you through targeted corrective exercises, and help you improve how you move—not just mask the symptoms.
Stop Living With IT Band Pain
Whether you're training for a race or just trying to get through the workday without pain, IT Band Syndrome can be disruptive, but it's absolutely treatable. The key isn’t just stretching or resting, it's understanding why the IT band is tight and retraining your body to move in a healthier, more balanced way.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.