Often, it starts subtly. You might notice a small lump in the palm of your hand. It isn’t painful, but it's firm and a little odd. Then you start to notice you're struggling to lay your hand flat on a table, or your fingers don’t extend like they used to when you stretch. Gripping a steering wheel, shaking hands, or even putting gloves on begins to feel different. Over time, one or more of your fingers start to curl inward toward the palm. This is often how Dupuytren's Contracture begins. A subtle, creeping change that slowly starts to change your hand function and your daily routine.
What Is Dupuytren's Contracture?
Dupuytren's Contracture is a hand condition where the tissue beneath the skin of your palm thickens and tightens over time. This fibrous tissue, known as fascia, can form cords that pull one or more of your fingers into a bent position. Once a finger is bent, it may not straighten fully, limiting your ability to perform daily activities.
Dupuytren's Contracture most commonly effects the ring and little fingers and usually progresses slowly over months or even years. Though not typically painful, it can significantly impact your hand function and quality of life.
Symptoms of Dupuytren's Contracture
Symptoms of Dupuytren's Contracture tend to develop gradually. Many people don’t notice anything is wrong until the condition has significantly progressed.
Nodules: Small, firm lumps in the palm that may feel tender early on.
Cords: Thickened tissue under the skin that may appear like a rope or string pulling the finger down.
Difficulty with daily tasks: Trouble placing the hand flat on surfaces, putting on gloves, or shaking hands.
Contracture: Fingers, especially the ring and little fingers, begin to bend toward the palm and can’t be fully straightened.
Causes of Dupuytren's Contracture
The exact cause of Dupuytren's Contracture is still not fully understood, but several contributing factors are known. It seems to be a combination of genetic and environmental triggers that lead to the thickening of connective tissue in the hand.
Contributing factors for developing Dupuytren's Contracture:
Genetics: A strong family history suggests a hereditary link.
Age: Most common in people over 50.
Gender: Men are more likely to develop it than women.
Ancestry: People of Northern European descent have a higher risk.
Lifestyle factors: Alcohol use and smoking have been linked to increased risk.
Can You Prevent Dupuytren's Contracture?
Unfortunately, there is no guaranteed way to prevent Dupuytren's Contracture, especially if you have a strong genetic predisposition. However, managing certain lifestyle choices may help reduce the risk or delay its onset.
Avoid smoking: Smoking is linked to blood vessel constriction, which may influence tissue changes.
Limit alcohol: Excessive alcohol intake may increase risk.
Control diabetes: Dupuytren's is more common in people with diabetes, so maintaining good blood sugar control may help.
Is Dupuytren's Contracture Genetic?
Yes, Dupuytren's Contracture is strongly linked to genetics. If you have a family history of the condition, you have a higher chance of developing it. It is often referred to as a hereditary condition, especially prevalent among those of Northern European ancestry.
This doesn’t mean you’re guaranteed to develop it, but you may want to keep an eye out for early signs and consult a healthcare provider if you notice symptoms.
What Helps Dupuytren's Contracture?
While Dupuytren's Contracture cannot be cured entirely, several treatments and management strategies can help maintain hand function and slow progression.
Stretching and hand therapy: Gentle exercises may improve flexibility in early stages.
Splinting: In some cases, night splints may be recommended to keep fingers extended.
Steroid injections: Can reduce inflammation in early stages.
How to Treat Dupuytren's Contracture
When the condition begins to interfere with your hand function, more active treatments may be helpful. These treatments for Dupuytren's Contracture can range from minimally invasive procedures to surgery.
Surgery (fasciectomy): In more severe cases, the thickened tissue is surgically removed.
Needle aponeurotomy: A needle is used to break the cords of tissue causing finger contraction.
Enzyme injections (collagenase): An enzyme is injected to soften and break down the cords.
What Makes Dupuytren's Contracture Worse?
Several factors may accelerate the progression or severity of Dupuytren's Contracture. Understanding these can help you avoid worsening the condition.
Ignoring symptoms: Delaying treatment can make eventual correction more difficult.
Injury to the hand: Trauma may exacerbate symptoms.
Smoking and heavy alcohol use: Both are associated with higher risk and more aggressive progression.
Do Certain Careers Make Dupuytren's Contracture More Likely?
Overuse or certain jobs have not been definitively proven to cause Dupuytren’s Contracture. While it might seem like repetitive hand use or manual labor is the culprit (especially because many people who do physical work notice the symptoms), research hasn’t confirmed a direct cause-and-effect link.
Some people used to think Dupuytren’s Contracture was mostly a problem for manual laborers because of things like hand strain or using vibrating tools. But more recent research shows it can affect anyone, no matter what kind of job they have, even people who work at desks all day. Physical work might make the symptoms show up sooner, but it doesn’t actually cause the condition. If anything, overusing your hands once Dupuytren’s has started might make it worse, but it’s not the root cause.
Making practical adjustments to your daily activities can help you maintain your independence and comfort as you manage Dupuytren's Contracture.
Modify tools and grips: Use ergonomic handles and adaptive devices for easier grip.
Stay active: Gentle hand stretches and overall fitness support circulation and mobility.
Monitor for progression: Regularly assess hand function and stay in touch with a provider.
When to See an Orthopedic Hand Specialist for Dupuytren's Contracture
If you notice any signs of finger contracture or thickened tissuein your palm, you should see a hand specialist. Early diagnosis can lead to better treatment outcomes.
Signs it’s time to see a specialist:
You can’t lay your hand flat on a table.
You notice visible cords or lumps.
Daily tasks like writing or grasping are becoming difficult.
How a Hand Specialist Diagnoses Dupuytren's Contracture
Diagnosis usually involves a physical examination. An orthopaedic hand specialist will assess the flexibility of your fingers and look for nodules or cords in the palm.
What the evaluation includes:
Tabletop test: You try to lay your hand flat on a table.
Palpation: The doctor feels for cords and nodules.
Range of motion: They assess how far you can move your fingers.
Yes, while there is no cure, Dupuytren's Contracture is treatable. With appropriate care, many people regain much of their hand function or prevent further deterioration. Early intervention is often key.
Treatment outcomes vary based on the severity of the condition and the method used. Some treatments offer lasting relief, while others may need to be repeated.
The Future with Dupuytren's Contracture
Living with Dupuytren's Contracture can be manageable with awareness and timely care. Many people continue to live active, fulfilling lives with the help of therapy, medical treatments, and modifications. Emerging therapies and surgical techniques continue to improve outcomes.
Stay informed, stay proactive, and don’t hesitate to seek help when changes begin.
What Not to Do If You Have Dupuytren's Contracture
Avoiding certain actions can help prevent further damage or worsening of the condition.
Do not ignore changes: Early symptoms matter.
Avoid forceful stretching or self-treatment: This can injure tissue.
Don’t skip follow-ups: Regular monitoring can catch progression early.
Avoid smoking and excessive alcohol: Both contribute to worsening the condition.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
At Princeton Orthopaedic Associates, your journey to better mobility and less pain doesn't end at the clinic doors. We’re thrilled to now offer Prescribe FIT, an innovative, insurance-covered virtual health coaching program that brings real, lasting change right to your home.
Whether you’re preparing for surgery, recovering from one, or simply hoping to reduce joint pain and improve your lifestyle, Prescribe FIT was made with you in mind.
What Is Prescribe FIT?
Prescribe FIT is more than just a health coaching program; it’s a partnership. You are paired with your own dedicated health coach, who works one-on-one with you to support healthier eating habits, consistent physical activity, and other simple lifestyle changes that can have a significant impact on orthopedic health.
This isn’t a one-size-fits-all solution. Your health coach will tailor each step to your unique goals, challenges, and daily routines, helping you stay motivated, on track, and supported every step of the way.
Why It Matters for Orthopaedic Health
Musculoskeletal (MSK) conditions like osteoarthritis, back pain, joint injuries, and post-surgical recovery are deeply affected by lifestyle habits. For many patients, weight loss and increased mobility are essential to reducing joint stress and chronic discomfort.
With Prescribe FIT, you can:
Alleviate daily joint pain
Improve strength and flexibility
Increase energy and stamina
Support better outcomes before and after surgery
Prevent future orthopedic issues from developing
And the best part? You do it all from the comfort of your home, with expert support just a phone call or message away.
Covered by Insurance? Yes, Really!
We believe that better health should be accessible to everyone. That’s why Prescribe FIT is covered by Medicare, Medicaid, and most major commercial insurers. Our friendly POA team will help you verify your eligibility and explain any financial responsibilities up front, so you can focus on your health, not the paperwork.
Ready to Begin?
If you’ve been told weight loss or lifestyle changes could help your orthopedic condition, but you’re unsure where to start, Prescribe FIT is the perfect place. There’s no pressure, no crash diets, no complicated gym routines. Just real, achievable goals that help you feel better, move better, and live better.
At POA, we’re always looking for ways to expand your care beyond the exam room. Prescribe FIT is one more way we’re investing in your long-term wellness, because how you heal matters just as much as where you heal.
Ask your POA provider about Prescribe FIT at your next visit, or contact us today to learn more about enrollment.
Let’s take the first step, together.
Pain After A Pop In The Knee
An ACL tear typically occurs during sudden pivoting, awkward landings, or stops, which are common in sports such as basketball, soccer, and skiing. It usually starts with a moment, an awkward pivot during a pickup basketball game, a sudden stop on the soccer field, or landing just slightly wrong after a jump. You might feel a sharp pain, instability, or hear that telltale pop. You go down, maybe hoping it’s nothing, but your knee swells, and walking becomes difficult. That’s the moment many athletes, professional, weekend warriors, or even teenagers, begin their journey with an ACL tear.
Understanding how to recognize a minor knee issue needing minimal home treatment versus what may be an ACL tear can be critical to the proper treatment and the fastest path to healing.
What Is the ACL and Why Does It Matter?
Your knee is one of the most complex joints in your body, and the ACL is one of its most important components. It plays a huge role in keeping your knee stable and allowing you to move with confidence, whether you're sprinting down a field or simply walking downstairs.
The ACL (anterior cruciate ligament) is one of the four major ligaments in your knee, connecting your thigh bone (femur) to your shinbone (tibia). Its job is to stabilize the knee, especially during rotation, pivoting, and rapid direction changes. That makes it crucial for athletes, but also important for anyone who walks, runs, or climbs stairs.
When the ACL tears, it doesn’t heal on its own. And unlike muscles, ligaments don’t regenerate well without surgical reconstruction.
ACL Tear Symptoms: What You Might Experience
If you’ve injured your knee and are wondering if it’s your ACL, you’re not alone. Knowing what symptoms to look for can help you decide whether it’s time to see a doctor or get imaging.
Here’s what people often report:
A “popping” sound or sensation at the moment of injury
Immediate pain, sometimes severe enough to stop activity
Swelling that begins within a few hours
Instability or “buckling”, especially when trying to pivot or walk
Loss of full range of motion
Some people can walk after an ACL tear, especially once swelling subsides, but the knee often feels unstable. Grade 1 (mild) tears may feel like soreness and instability under stress, but they’re rare. By two weeks post-injury, swelling may reduce, but instability often persists.
Grade 3 (Complete tear): Surgical (ACL reconstruction) 6–12 months before full return to sport
MCL Tear Recovery:
Grade 1 (mild, stretching without tearing): 1–3 weeks
Grade 2 (moderate, partial tear): 3–6 weeks with bracing and PT
Grade 3 (complete): 6–10 weeks, may involve bracing or rare surgical repair
Why you can trust us:
We have multiple highly specialized, board-certified, fellowship-trained orthopaedic surgeons.
We know that we serve people - actual humans - not random orthopaedic conditions. That drives us to compassionate care.
The world of orthpaedics is constantly evolving. Our orthopaedic surgeons are constantly evaluating new techniques, tools and methods to serve our community even better.
We provide outcome-focused treatment. We work with our patients to achieve their goals, all while developing custom treatment plans that fit our patient's lives.
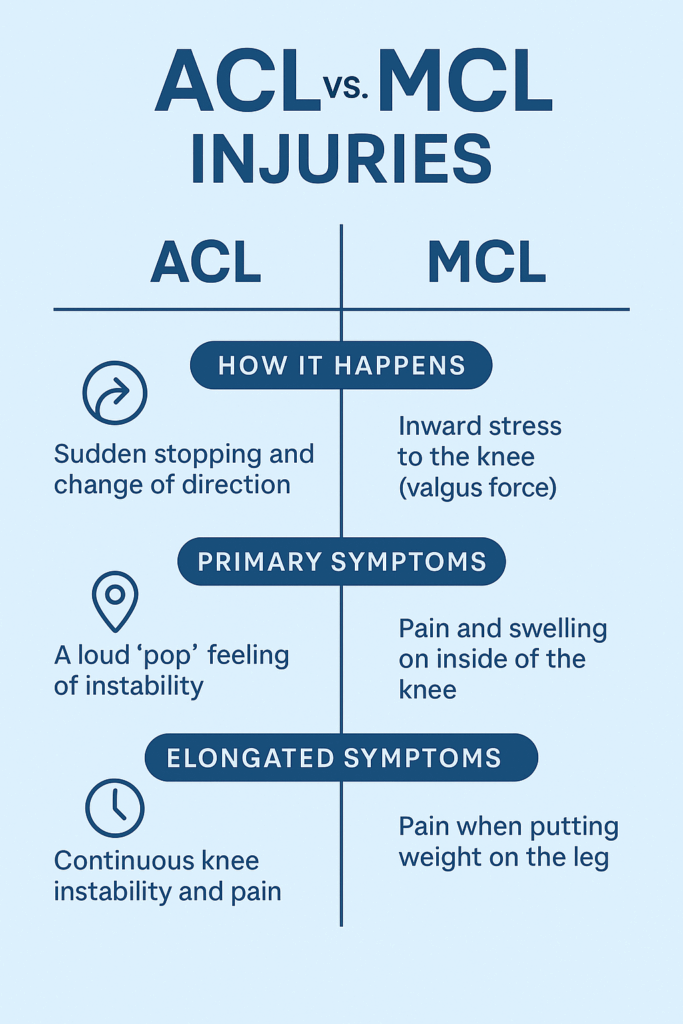
Knee injuries can be confusing because symptoms often overlap. The ACL and MCL are two different ligaments with different functions, injury mechanisms, and treatment approaches. Understanding the difference is critical for proper recovery.
Many people confuse ACL and MCL (medial collateral ligament) injuries. Here’s how an ACL tear and MCL tear differ:
ACL Tear
MCL Tear
Location
Inside the knee, central
Inside of the knee (medial side)
Mechanism
Pivoting, cutting, or landing
Direct blow to outer knee or overstretching
Sound
Often a pop
Less commonly a pop
Swelling
Fast and significant
Less severe swelling
Instability
Knee feels unstable or “gives out”
Usually more stiff than unstable
Healing Potential
Does not heal on its own
Often heals without surgery
First-line Treatment
Physical therapy or surgical reconstruction
Bracing, rest, and physical therapy
Surgery Needed?
Often required in active patients
Rarely required (unless Grade 3 + other injuries)
Return to Sport
6–12 months (after reconstruction)
4–12 weeks (depending on severity)
Key difference: An MCL tear can often heal with rest and bracing. An ACL tear usually won’t.
Can You Tear Both ACL and MCL at Once?
Yes, and this is more common than people think, especially in sports injuries. This is called a combined ligament injury and often involves the ACL, MCL, and/or meniscus. These cases require specialized surgical planning and longer rehabilitation timelines, making early diagnosis even more critical.
How to Know Which One You’ve Injured
While some clues (pain location, swelling speed, mechanism) may point toward one ligament over the other, you cannot reliably self-diagnose an ACL or MCL tear. Some people with a complete ACL tear are still able to walk or bend their knee, which can be misleading.
We recommend consulting one of our sports medicine specialists or an orthopedic knee surgeon as soon as possible. A timely and accurate diagnosis gives you the best chance of a full recovery and of avoiding chronic knee issues.
Adolescent ACL Tear vs. Adult ACL Tear
When it comes to ACL injuries, age matters. Kids and teens are still growing, and that can make treatment more complicated. What’s best for a 14-year-old soccer player may be very different from what’s recommended for a 30-year-old runner.
ACL injuries are increasing in adolescents, especially teenage athletes. The growth plates (areas of developing cartilage near the ends of long bones) in kids add complexity:
Non-surgical approaches may be prioritized in younger teens to avoid damaging growth plates.
Modified surgical techniques (like physeal-sparing procedures) are used if surgery is necessary.
Rehabilitation may need to be longer to protect future growth and return-to-play safely.
In adults, decisions are often based on lifestyle, activity level, and degree of instability.
Surgery isn't always required for an ACL tear, but it can often be recommended. Once you’ve torn your ACL, the big question is: Do you need surgery? The answer depends on your goals, age, activity level, and the nature of the tear. For some, physical therapy may be enough. For others, reconstruction is the most straightforward path back to full function. Your treatment path is specific to you, and our specialists will build a plan that meets the needs of your injury and desired recovery outcome.
Non-Surgical ACL Tear Treatment (select cases)
Mild (grade 1) sprains may recover within 3–6 weeks with rest and rehab.
For:
Low-demand lifestyle (non-athletes)
Partial tears
Older adults
No instability with daily activity
Approach:
Activity modification
Physical therapy to strengthen surrounding muscles (especially quads and hamstrings)
Bracing for certain activities
Surgical ACL Tear Treatment (Reconstruction)
Surgery may sound intimidating, but for many people, it offers the best chance at regaining full knee stability and returning to high-level physical activity. The procedure is common, safe, and continually improving.
Most active individuals, especially athletes or younger patients, choose ACL reconstruction. Here’s how it works:
Torn ACL is replaced with a graft (from your own hamstring, patellar tendon, quadriceps tendon, or a donor).
Surgery is typically minimally invasive (arthroscopic).
Recovery involves 6–12 months of guided physical therapy.
Factors influencing surgery:
Presence of other injuries (meniscus tear, cartilage damage)
Age and activity level
Desire to return to sports
Degree of instability
What Not To Do After an ACL Tear
Sometimes what you don’t do is just as important as what you do. The wrong move after an ACL tear can worsen the injury or lead to complications down the line.
Don’t ignore instability. Repeated “giving out” episodes can damage the meniscus or cartilage.
Don’t rush rehab. Returning to play too soon raises your risk of re-tear (or injuring the other knee).
Don’t skip the MRI. X-rays won’t show ligament damage. An MRI is needed to confirm the tear and check for other injuries.
Don’t rely solely on a knee brace if you're planning to return to sport, it doesn't replace ligament function.
Leaving an ACL tear untreated can lead to further joint damage, including cartilage wear or meniscus tears.
Can You Still Use Your Knee with a Torn ACL?
Some people can still walk, squat, or bend their knee shortly after tearing their ACL. However, without stability, these motions can cause further injury. If you suspect you have an ACL tear we recommend you see a orthopaedic specialist as soon as possible for a comprehensive evaluation.
Life After an ACL Tear: Hope, Patience, and Progress
An ACL tear is a detour, not a dead end. With the right care, commitment, and patience, people of all ages get back to running, jumping, and playing, often even better than before.
Tearing your ACL can feel like the end of your athletic identity, but it’s not. Thousands of people, from high school athletes to weekend hikers to pro players, successfully return to sports and active lifestyles every year.
The key is getting the right diagnosis, choosing the right treatment path for your goals, and committing to smart, structured rehab.
Diagnosis: Why You Need a POA Orthopaedic or Sports Medicine Specialist
While some symptoms can help differentiate between the two, it’s extremely difficult to diagnose knee ligament injuries accurately without imaging and specialist assessment.
Here’s why seeing a POA or orthopedic knee specialist is essential:
Physical tests (like Lachman or valgus stress test) must be performed with skill and interpreted in context.
MRI scans are required to confirm the exact ligament involved and assess associated injuries (meniscus, cartilage).
Misdiagnosis can delay proper healing. For example, treating an ACL tear like an MCL sprain could lead to long-term instability or joint damage.
Bottom Line: Always get a clinical evaluation with a knee specialist, especially if you heard a pop, felt instability, or have swelling. Don’t self-diagnose based on symptoms alone.
Meet Our Orthopaedic Knee Specialists
Can You Recover from an ACL Tear? Here’s What to Expect
Tearing your ACL may feel overwhelming, but it's not the end of your active lifestyle. Whether you're a competitive athlete or someone who just wants to move without fear, recovery is possible with the right approach. From early diagnosis and personalized treatment plans to structured rehab and return-to-play timelines, every step forward matters. Understanding your options is the first step toward getting back to what you love, with strength and confidence.
If you’re reading this, you may be worried about what’s next. Take a breath, you’re not alone. Understanding your injury is the first step toward healing. Now it’s time to take action. If you suspect an ACL tear, don’t wait. Get evaluated by a sports medicine physician or orthopedic specialist. Early diagnosis means earlier healing and a better chance of getting back to doing what you love.
ACL Tear vs. Meniscus Injury: Key Differences at a Glance
While both ACL and meniscus injuries are common in athletes and active individuals, they are very different in structure, symptoms, and recovery needs. Knowing the distinctions can help guide proper diagnosis and treatment.
How an ACL Tear and Meniscus Tear Happen
ACL Tear:
Typically from a sudden pivot, change in direction, or awkward landing
Often non-contact, though can also result from trauma
Common in sports like soccer, basketball, skiing
Meniscus Tear:
Often caused by twisting the knee while the foot is planted
Can occur with or without an ACL tear
May result from degeneration in older adults or a sharp movement in younger athletes
Primary (Immediate) Symptoms
Symptom
ACL Tear
Meniscus Tear
Popping Sound
Very common
May occur, but less dramatic
Swelling
Rapid (within hours)
Gradual (over 24–48 hours)
Instability
Knee may "give out"
Usually feels stable
Pain Location
Deep or central knee
Side or back of knee (depending on tear location)
Mobility
Loss of motion due to swelling and instability
May still walk, but discomfort with twisting/squatting
Prolonged/Chronic Symptoms (If Left Untreated)
Symptom
ACL Tear
Meniscus Tear
Knee Giving Out
Frequent instability, especially during pivoting
Rarely unstable
Locking or Catching
Uncommon
Very common — knee may catch or lock during motion
Grinding or Clicking
Occasionally
Common, especially with movement
Degeneration Risk
Higher if combined with meniscus injury
Increases risk of arthritis over time
Return to Activity
Difficult without surgery for active individuals
Sometimes possible without surgery, depending on severity and tear location
A meniscus tear often presents with joint line tenderness and mechanical symptoms (like locking), while an ACL tear leads to feelings of instability and swelling shortly after injury. However, since both can coexist, and symptoms can overlap, accurate diagnosis with an MRI and specialist evaluation (by a POA or orthopedic physician) is essential. Read more about meniscus tears.
Quick Overview
ACL
Meniscus
Function
Stabilizes the knee
Cushions and supports joint movement
Injury Type
Ligament
Cartilage
Instability?
Yes
Rarely
Locking
Rare
Common
Needs Surgery
Often (for active patients)
Sometimes, depending on tear type
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
Tweaked your knee, but the pain isn't going away?
You were mid-pivot, chasing a ball or turning to grab something behind you, when a sharp pop hit your knee. Not loud, but distinct. You paused, unsure if it was serious. Maybe just a tweak, you thought. But within hours, the swelling crept in, the joint stiffened, and walking suddenly felt unfamiliar. That small twist? It turned into something much bigger.
That moment likely marked the beginning of a meniscus tear—a common yet disruptive injury affecting the cartilage in your knee. Whether it's from a sudden injury or years of wear and tear, the result is often the same: pain, limited movement, and questions about what comes next.
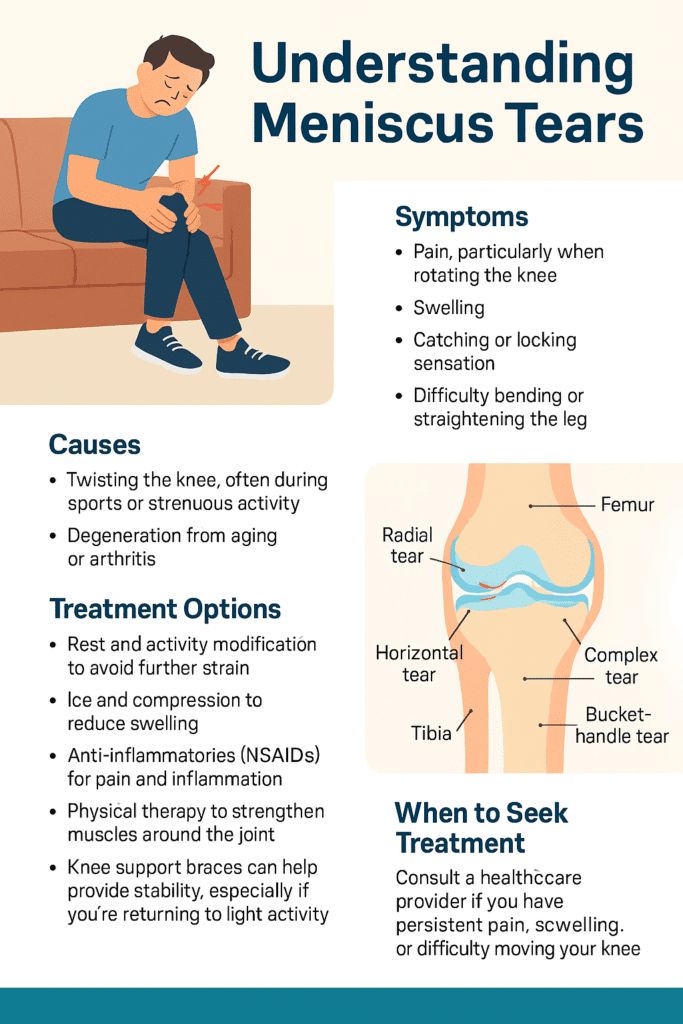
What Is a Meniscus Tear?
Inside each of your knees are two rubbery, wedge-shaped pieces of cartilage: the medial and lateral menisci. These act like shock absorbers between your thighbone and shinbone, helping to distribute weight and stabilize movement. A tear occurs when this cartilage is damaged—usually from twisting motions or degeneration over time.
You don't have to be an athlete for this to happen. A quick squat, an awkward turn, even standing up too fast with pressure on the joint can be enough, especially if the cartilage is already weakened with age.
Common Causes
There are two primary culprits behind a torn meniscus:
Trauma or sudden movement, like twisting or pivoting during sports, or while playing with your kids!
Degeneration, where age-related wear and tear thins and weakens the cartilage, making it easier to tear with minor movements.
Both scenarios are incredibly common. Lifting a heavy box incorrectly or kneeling on a hard surface for too long can be all it takes.
Meet Our Orthopaedic Knee Specialists
Symptoms of a Meniscus Tear
The first few hours after the tear are often the most telling. At first, discomfort may be the only symptom of a meniscus tear you might feel. Or, the only symptoms of a meniscus tear present at first are just a dull, persistent ache, made worse by movement. You might feel fine while sitting, but as soon as you try to walk or bend, your knee doesn't cooperate. Some describe it as a "stuck" sensation, where the joint feels like it won't fully extend or flex without pain or resistance. But then the pain deepens, swelling begins, and your range of motion shrinks even more.
Clicking, popping, or catching during movement can also indicate a torn flap of cartilage catching in the joint. Check out this post to read more about the Types of Meniscus Tears.
Additional Symptoms of a Meniscus Tear:
Locking, catching, or the feeling of instability
Sharp or aching pain, often on the inner (medial) side of the knee
Swelling that develops gradually
A popping sound or sensation during injury
Difficulty straightening or bending the knee
If you're looking for clarification on the symptoms of a meniscus tear, you are not alone. Many people deal with a torn meniscus and don't realize the seriousness until the stiffness and pain don't go away.
Do You Need to See a Doctor For a Meniscus Tear?
If you're hoping it will just go away, consider this: untreated meniscus tears can worsen over time, leading to more pain and even long-term joint issues like osteoarthritis.
Seek professional help if:
Pain persists beyond a few days
Swelling continues or worsens
You experience locking, buckling, or instability
You can't put normal weight on the leg
Ignoring it risks further tearing or cartilage breakdown. Early diagnosis often means better, less invasive treatment options.
Why you can trust us:
We have multiple highly specialized, board-certified, fellowship-trained orthopaedic surgeons.
We know that we serve people - actual humans - not random orthopaedic conditions. That drives us to compassionate care.
The world of orthpaedics is constantly evolving. Our orthopaedic surgeons are constantly evaluating new techniques, tools and methods to serve our community even better.
We provide outcome-focused treatment. We work with our patients to achieve their goals, all while developing custom treatment plans that fit our patient's lives.
A physical exam can often provide early clues. A clinician will test your range of motion and apply gentle pressure or rotation to identify pain points. In many cases, imaging, like an MRI, is used to confirm the diagnosis and pinpoint the severity and location of the tear.
Meniscus Tear Remedy
Not all meniscus tears require surgery. If you're looking for a meniscus tear remedy, treatment depends on the type of tear, location, and severity of the tear, as well as your activity level and age.
Conservative Meniscus Tear Remedy Approaches:
Rest and Activity Modification
One of the first things you can do is to give your knee a break! If you are able to identify them, avoid movements thatmake the pain worse. Common ones include twisting, squatting, or any high-impact activities. Resting allows the damaged cartilage in your knee to settle and inflammation to subside which gives your body a chance to begin healing. This doesn't mean you have to be totally immoble, but be mindful of your movements and eliminate anything that causes discomfort or strain.
Ice and Compression
Applying ice packs to your knee helps reduce swelling and numbs the area, easing the pain. Aim for 15–20 minutes every few hours in the first few days. Pair this with a compression bandage or sleeve to minimize inflammation and support the knee structure. Together, they help control the body's inflammatory response and provide short-term relief while preventing further irritation.
Anti-inflammatories (NSAIDs)
Over-the-counter medications like ibuprofen (Advil) or naproxen (Aleve) can significantly reduce inflammation and help manage pain. These drugs target the body’s natural inflammatory chemicals, making it easier to move the joint and complete daily activities without aggravating the tear. Always follow dosage instructions and consult your doctor if you’re taking them for more than a few days.
Physical Therapy
Once the pain and swelling are under control, targeted exercises become essential. A physical therapist will guide you through movements designed to strengthen the muscles surrounding your knee—especially the quadriceps and hamstrings. This not only speeds up recovery but also restores joint stability, improves flexibility, and reduces the risk of re-injury.
Knee Support Braces
A well-fitted knee brace offers additional stability, particularly when walking or performing light activities. Braces help limit unwanted lateral movement and protect the joint during recovery. If your knee tends to feel unstable or you're easing back into exercise or work, wearing a brace can provide the support and confidence you need to move safely.
Small tears near the outer edge, where the blood supply is richer, often heal with conservative care.
Surgical Options:
If the tear is large, causes locking, or doesn't improve, arthroscopic surgery may be recommended. Options include:
Meniscus repair (stitching the cartilage back together)
Partial meniscectomy (removing the torn section)
Total meniscectomy (rare and typically avoided)
Surgery is more likely in younger, active individuals or when the tear is in a critical area.
Torn Meniscus Recovery Timeline
How long it takes a torn meniscus to heal depends entirely on the treatment path and your consistency with rehab. Below is a general idea of recovery times based on the type of treatment - this is for reference only and not a diagnosis and treatment.
Treatment Method
Est. Recovery Time
Conservative (rest, PT)
4-8 weeks
Partial Meniscectomy
4-6 weeks
Arthroscopic Repair
3-6 months
So, how long does it take for a meniscus tear to heal? It may take time to regain strength and trust in your knee even after healing.
Meniscus Tear Common Questions
Can You Walk With a Meniscus Tear?
Yes—but that doesn't mean you should. Many people are able to walk with a torn meniscus, especially if the pain is mild. But without proper treatment, walking on a torn meniscus can cause further damage or transform a minor tear into a more serious one.
If you must stay mobile, supportive bracing and avoiding twisting motions is essential.
What Does a Torn Meniscus Look Like on The Outside
Despite the pain and swelling, a torn meniscus often doesn't present visible signs like bruising or discoloration. That's why if you're looking for answers to "what does a torn meniscus look like on the outside," the truth is, it doesn't look like much so you won't find much. The damage is internal; symptoms often show through movement limitations and experienced pain, not appearance.
How to Prevent a Meniscus Tear
Prevention of a meniscus tear isn't just about avoiding sports injuries—it's about daily movement, posture, and support.
Smart Prevention Strategies:
While it's no guarantee you'll avoid having a torn meniscus, there are some smart prevention strategies! Some strategies include:
Warm up: Before starting any physical activity, properly warm up to loosen up your muscles in preparation for the activity.
Stretch regularly: Regularly stretching, especially the hamstrings and calves, can also be helpful.
Strengthen: Doing strengthening work on leg muscles (quads, glutes, hamstrings) helps to improve stability. You'll want to avoid deep squats or twisting under load
Knee supports: If you know you're prone to injury or returning from one, wearing knee supports can be beneficial to prevent a meniscus tear.
You don't need to be an athlete to tear your meniscus—and you don't need to live with the pain either. Even activities like walking the dog or playing with your kids carry risk if you're not mindful of sudden directional changes! With awareness, early action, and proper care, recovery is possible and often complete. Pain-free movement starts with taking your symptoms seriously, getting the right diagnosis, and committing to healing fully.
If it feels wrong, it probably is. Trust your body, and give it what it needs to bounce back. Contact us today to schedule with one of our specialists.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
Your hip pain might be hip flexor pain!
You wake up in the morning and swing your legs over the edge of the bed. Before your feet even hit the floor, there it is—a deep, nagging tightness at the front of your hip. Walking to the kitchen feels stiff, almost like your legs are moving through molasses. You stretch instinctively, but it doesn’t quite hit the spot. When you sit down with your coffee, the ache creeps back in. Sitting at your desk later, the discomfort becomes sharp, pulling with every shift in position. Going for a jog—something that used to energize you—now leaves your hips feeling locked up, like rusty hinges refusing to swing open. This is life with tight hip flexors: a quiet, persistent thief of your freedom of movement.
For many adults, especially those with desk jobs or active lifestyles, hip pain can sneak in gradually and eventually become a daily discomfort. Having tight hip flexors is one of the most common culprits. Whether you spend hours sitting at a computer or you're constantly on the move, running or cycling, your hip flexors may be working overtime—and not always in a good way. Understanding how hip flexor tightness develops, and more importantly, how to alleviate it, is key to maintaining healthy, pain-free movement.
What Are the Hip Flexors?
The hip flexors are a group of muscles located at the front of your hips that play a vital role in nearly every lower body movement. These muscles allow you to lift your knee toward your chest, bend at the waist, and stabilize your pelvis during standing, walking, and running.
The key muscles in the hip flexor group include:
Iliacus and Psoas Major (Iliopsoas): These powerful muscles originate in your pelvis and lower spine and insert into your upper thigh, working together to lift your leg and maintain trunk stability.
Rectus Femoris: This muscle is part of the quadriceps group and assists with both hip flexion and knee extension.
Sartorius: The longest muscle in the human body, it runs from the outer hip across the thigh to the inner knee, aiding in hip flexion, abduction, and external rotation.
These muscles work together to allow fluid motion, but when overworked or underused, they become shortened and tight, resulting in limited mobility and discomfort.
Why you can trust us:
We have multiple highly specialized, board-certified, fellowship-trained orthopaedic surgeons.
We know that we serve people - actual humans - not random orthopaedic conditions. That drives us to compassionate care.
The world of orthpaedics is constantly evolving. Our orthopaedic surgeons are constantly evaluating new techniques, tools and methods to serve our community even better.
We provide outcome-focused treatment. We work with our patients to achieve their goals, all while developing custom treatment plans that fit our patient's lives.
Hip flexor tightness often arises from a combination of inactivity and muscular imbalance, and in some cases, overuse.
Common causes of hip pain from tight hip flexors include:
Prolonged Sitting: Sitting for extended periods—at a desk, in a car, or on the couch—keeps the hip flexors in a shortened position. Over time, this leads to adaptive shortening and chronic tightness.
Repetitive Activity: Runners, cyclists, and athletes performing frequent leg lifts use their hip flexors intensively. Without adequate recovery and stretching, this overuse causes the muscles to become stiff and inflamed.
Muscle Weakness: Weakness in the glutes, deep core muscles, and stabilizers like the piriformis shifts the workload to the hip flexors, which are not designed to handle prolonged stabilization. This compensation pattern leads to over-recruitment and tightness.
Poor Posture or Pelvic Alignment: Anterior pelvic tilt (a common postural issue where the pelvis tilts forward) places the hip flexors in a shortened state even while standing.
What Happens When the Hip Flexors Become Tight?
When you have tght hip flexors it can reduce the range of motion in your hips, cause pelvic misalignment, and place strain on the lower back. You might feel discomfort in your groin, stiffness in the front of your hip, or even aching pain during or after activity. Long-term tightness can lead to:
Lower back pain
Decreased athletic performance
Changes in walking mechanics
Pelvic instability
Pain radiating into the thigh or knee
If this issues is lefft unaddressed, this tightness becomes more than a nuisance to you—it becomes a chronic issue that impacts every step, sit, and stride.
Hip Flexor Pain
Hip flexor pain is most commonly felt in the front of the hip and upper thigh, but it can also radiate to other nearby areas depending on the severity, cause, and specific muscles involved.
Here’s a breakdown of where and how hip flexor pain is typically experienced:
Primary Hip Flexor Pain Location
Front of the hip (anterior hip):
This is the most common location. It may feel like a deep ache or sharp pinch where your thigh meets your pelvis, especially when lifting your knee, walking uphill, or standing after sitting.
Upper thigh:
Pain can extend downward along the front of the thigh, particularly if the rectus femoris (a dual-function hip and knee flexor) is involved.
Associated Hip Flexor Pain Areas
Groin area:
If the iliopsoas is especially tight or inflamed, pain may be felt deep in the inner hip or groin.
Lower back:
Because the psoas muscle attaches to the lumbar spine, chronic tightness or spasms can lead to referred pain or tension in the lower back.
Pelvis or sacroiliac (SI) region:
Misalignment caused by tight hip flexors can lead to pain around the SI joints or pelvic rim.
Anterior knee:
In some cases, overuse of the rectus femoris can cause discomfort that tracks down toward the knee.
Hip Flexor Pain Triggers
Rising from a seated position
Prolonged sitting or standing
Running, cycling, or stair climbing
Lunges or high-knee movements
Lying flat without support under knees (for severe cases)
If the pain is sharp, persistent, or affects your ability to walk or move normally, it may be a sign of a strain, tendonitis, or labral issue—warranting a visit to an orthopedic specialist or physical therapy.
How to Prevent Hip Flexor Problems
Prevention goes beyond stretching. It involves a comprehensive movement and strength strategy to ensure the hip flexors are neither overloaded nor neglected:
1. Take Frequent Movement Breaks
Set a timer to stand and walk every 30–45 minutes.
Try standing meetings or a sit-to-stand desk if your job is sedentary.
Walk during phone calls, stretch between tasks, and avoid long static postures.
3. Strengthen Supporting Muscles
Glute bridges, clamshells, side leg raises, and deadlifts strengthen the posterior chain, reducing reliance on the hip flexors.
5. Core stabilization:
Working strengthening exercises into your routine, such as planks and bird-dogs, prevents the spine and pelvis from wobbling. They also help stabilize your core, which takes pressure off the hips.
2. Maintain Proper Posture
Avoid slumping while seated. Sit upright with hips and knees at 90 degrees.
Engage your core and glutes when standing to maintain a neutral pelvic position.
4. Incorporate Mobility Work Into Your Routine
Dynamic warm-ups before exercise and controlled hip mobility drills (like leg swings and hip circles) keep the hip joint nourished and flexible.
Foam rolling the quads and lower back can help release tight fascia around the hip.
Home Treatment of Tight Hip Flexors
If you're already dealing with symptoms of tightness, there are ways you can find relief. It's beneficial to take a multi-pronged approach:
Use Heat Therapy before stretching to increase circulation.
Perform static and dynamic stretches daily, focusing on consistency over intensity.
Improve neuromuscular control by re-training movement patterns—walk mindfully, stand tall, and avoid hip “gripping.”
Four Hip Flexor Stretches to Relieve Tightness
Hip flexor stretches done at home help restore flexibility and mobility in the front of the hips, reducing stiffness from prolonged sitting or repetitive activity. Regular stretching can alleviate pain, improve posture, and enhance movement efficiency during daily activities or workouts. Additionally, it supports pelvic alignment and reduces strain on the lower back by balancing muscle tension across the hip complex.
These evidence-based stretches are simple, safe, and effective. Perform them twice daily, holding each for 30–60 seconds per side, and repeat for 2–3 sets.
1. Half-Kneeling Hip Flexor Stretch
This stretch helps open the hip while promoting glute engagement.
Instructions:
Kneel with your left knee on the ground and right foot forward.
Contract your glutes and gently tilt your pelvis under.
Shift forward until you feel a stretch in the left hip.
For more intensity, raise your left arm overhead and lean slightly right.
2. 90/90 Hip Mobility Stretch
Improves rotational mobility of the hip joint.
Instructions:
Sit with your right leg in front, bent 90 degrees, and your left leg out to the side in the same position.
Sit upright and lean slightly forward without collapsing your chest.
Feel the stretch in the outer hip and groin. Switch sides.
3. Supine Hip Flexor Bed Stretch
Uses gravity to gently open the hip flexors.
Instructions:
Lie on your back on the edge of a bed with your right leg hanging off.
Keep the left knee bent and foot flat on the bed.
Pull the left knee gently toward your chest while letting the right leg dangle.
4. Side-Lying Quad & Hip Flexor Stretch
Targets both the front thigh and deeper hip structures.
Instructions:
Lie on your left side, knees bent.
Reach your right hand behind to grab your right ankle.
Gently pull your foot toward your glutes while keeping your spine neutral and pelvis tucked.
When to See a Specialist
While stretching and strengthening can resolve many cases of tightness, persistent or worsening pain should not be ignored. You should seek care if you experience:
Pain that radiates into the thigh or groin
Hip pain lasting longer than two weeks
Snapping, catching, or grinding sensations
Instability or weakness in the hip
Inability to perform daily tasks like walking or climbing stairs without pain
The Right Specialist to See:
If you are experiencing persistent or worsening hip flexor pain like those just mentioned, it's important you see a specialist for an evaluation. At Princeton Orthopaedic Associates, we have multiple specialists who can help with your hip flexor pain. Contact us to schedule an appointment.
Orthopedic Doctor: A specialist in musculoskeletal conditions who can diagnose underlying joint or soft tissue problems.
Sports Medicine Doctor: Ideal for active individuals or athletes with hip flexor injuries related to overuse or movement patterns.
Physical Therapist: Offers personalized rehabilitation programs, manual therapy, and neuromuscular re-education for tight or injured hip flexors.
Tight hip flexors don’t just affect how your hips feel—they influence your spine, posture, gait, and overall comfort. They can sideline your fitness, sap your energy, and even cause pain elsewhere in the body. Fortunately, with the right combination of movement, strengthening, and stretching, you can restore mobility and function to your hips. Don’t let tight muscles limit your life—take action early and seek professional care when needed.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
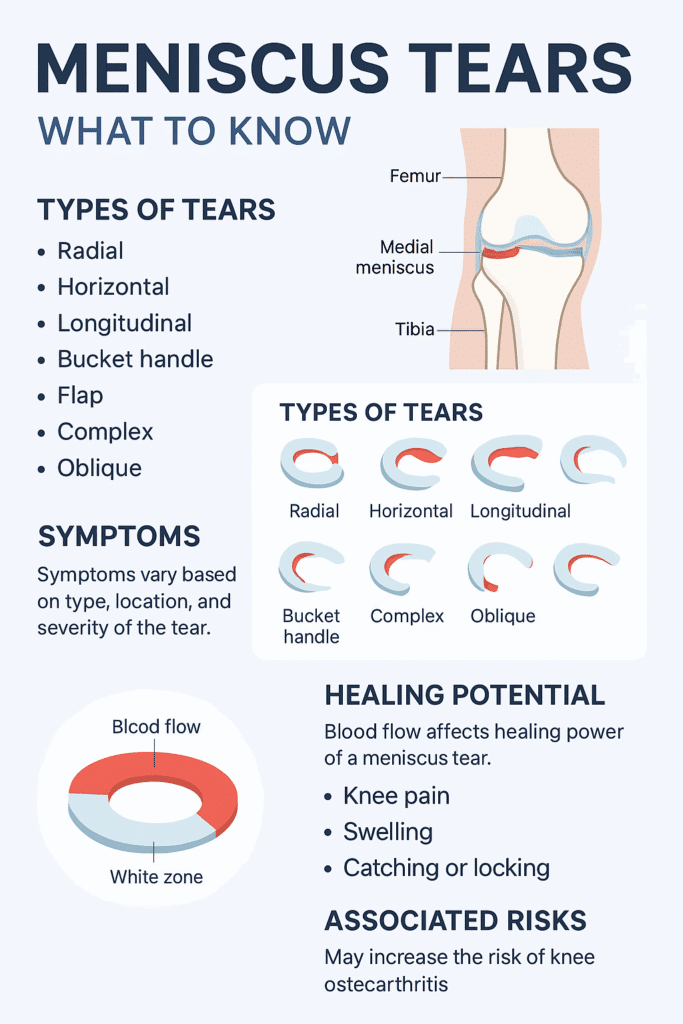
Meniscus tears are classified based on tear shape and tear location. This classification helps determine whether the injury may heal with rest and therapy or if it needs surgical treatment. If you're looking to understand the type of tear you have, we have broken them down below:
Meniscus Tear Shapes
1. Meniscus Radial Tear
A radial tear cuts straight across the meniscus from the inner edge toward the outer rim, similar to the spoke of a wheel. These are common and usually occur in areas with poor blood flow, which limits the body’s ability to heal the tear on its own. Treatment often involves trimming the damaged section.
2. Meniscus Horizontal Tear
A horizontal tear runs between the upper and lower layers of the meniscus, dividing it in half like a sandwich. These tears are more common in older adults and may be repairable if located in the outer region of the meniscus, where blood supply is better.
3. Meniscus Vertical (Longitudinal) Tear
This tear runs lengthwise along the curve of the meniscus, following its C-shape. It is often seen in younger, athletic individuals and may respond well to surgical repair, especially when located in the outer third of the meniscus.
4. Meniscus Bucket Handle Tear
A bucket handle tear is a severe form of a vertical tear. In this case, a large portion of the meniscus flips inward into the knee joint, making it difficult to bend or straighten the knee. It often causes locking and typically requires surgery to correct.
5. Meniscus Flap Tear
A flap tear results in a loose piece of cartilage that creates an uneven edge. This flap may shift with knee motion, causing clicking, catching, or locking. If symptoms are persistent, the loose section is often trimmed during a minor procedure.
6. Meniscus Complex Tear
A complex tear includes multiple tear patterns—usually both radial and horizontal—and often occurs in worn or degenerated menisci. These are difficult to repair and typically require removal of the damaged sections.
7. Meniscus Oblique (Parrot Beak) Tear
An oblique tear forms at an angle, creating a curved flap that resembles a parrot’s beak. The flap can catch in the joint and lead to sharp pain or instability. Surgical trimming is often used if the tear is unstable.
Meniscus Tear Locations
In addition to the shape of the tear, the location is a major factor in symptoms and treatment decisions. These are the meniscus tear locations:
Medial meniscus tear – inside of the knee
Lateral meniscus tear – outside of the knee
Posterior horn tear – back portion of the meniscus
Anterior horn tear – front portion of the meniscus
Meniscus root tear – where the meniscus anchors to the bone
Each location has different mechanical demands, and tears in different areas may feel different or affect how the knee moves.
Location and Healing Potential
The meniscus has three zones based on blood supply that affect how well a tear can heal:
Red zone (outer third) – good blood supply; better chance of healing on its own or after repair
White zone (inner third) – poor blood flow; limited natural healing
Red-white zone (middle third) – transitional; healing depends on tear size and stability
Long-Term Effects of Untreated Meniscus Tears
How long does it take a meniscus tear to heal? The answer is, it depends. However, if a torn meniscus is left untreated or heals poorly, it can lead to:
Chronic knee instability
Frequent swelling and inflammation
Faster joint cartilage breakdown
Higher risk of developing osteoarthritis
Early diagnosis, combined with the right treatment approach, helps protect long-term knee function and mobility.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
Chronic Pain Isn't In Your Head
Living every day in pain can be debilitating. Imagine waking up each morning already exhausted—not because you didn't sleep, but because your pain kept you tossing and turning all night. Your back aches the moment your feet hit the floor. You grip the bathroom sink for support while brushing your teeth, and getting dressed feels like running a marathon. Driving to work takes every ounce of concentration, not just because of traffic but because your joints throb with every turn. Meetings blur as you shift in your seat, trying to find a less painful position. By the time you get home, you're too sore to cook dinner, too drained to enjoy time with family, and overwhelmed by the idea of another night spent battling discomfort.
This is what daily life can feel like if you're living with chronic pain but it doesn't have to stay this way.
The Serious Impact of Living With Chronic Pain
Chronic pain doesn't just hurt your body. It reshapes your life in ways most people never see.
Physical Decline from Chronic Pain
Pain discourages movement, leading to muscle atrophy, joint stiffness, and reduced endurance.
Emotional Strain from Chronic Pain
Constant discomfort takes a toll on mental health, often triggering depression, anxiety, and social withdrawal.
Sleep Disruption from Chronic Pain
Pain can make it difficult for you to fall asleep or stay asleep, leaving you fatigued and foggy during the day.
Career Limitations from Chronic Pain
Reduced mobility, frequent doctor visits, and cognitive distraction can affect work performance and job retention.
Strained Relationships from Chronic Pain
Chronic pain can make you less active, irritable, or dependent on others, placing stress on personal and family dynamics.
Meet our Physiatry Experts
Top 5 Most Common Chronic Pain Conditions
1. Chronic Back Pain
Lower back pain can stem from degenerative disc disease, where the discs between vertebrae lose their cushioning, or herniated discs that press on nerves. Strains, poor posture, or conditions like arthritis and spinal stenosis also contribute.
Symptoms of Chronic Back Pain:
Dull or Sharp Pain in Your Lower Back
This can feel like a constant ache or a sudden stabbing pain that worsens with movement.
Stiffness or Reduced Flexibility
You may struggle to bend, twist, or stand upright after sitting or sleeping.
Radiating Pain into the Buttocks or Legs
This often signals nerve involvement, such as sciatica.
Pain That Worsens With Activity or Prolonged Sitting
Common with desk jobs or long commutes, even mild activity may worsen discomfort.
Muscle Spasms
Sudden tightening of muscles may occur, making movement painful or unpredictable.
How a Pain Management Doctor Can Help:
At POA, we begin with diagnostic imaging and a detailed physical assessment to determine the exact cause of lower back pain. Treatment plans are individualized and may include physical therapy to strengthen core muscles, medication management, and targeted injections. For persistent cases, minimally invasive procedures such as radiofrequency ablation can provide long-term relief.
Options may include:
Epidural steroid injections
Facet joint injections
Core stabilization therapy
Radiofrequency nerve ablation
2. Chronic Pain Because of Osteoarthritis (OA)
OA is primarily due to the gradual breakdown of cartilage in joints over time. Risk factors for osteoarthritis include age, obesity, prior joint injuries, and repetitive stress from work or sports.
Symptoms of Osteoarthritis (OA):
Joint Pain, Especially After Movement
Pain that worsens with activity and improves after rest.
Swelling and Tenderness
Inflammation causes visible swelling and sensitivity in the joint.
Reduced Range of Motion
Stiff joints limit how far or freely you can move.
Joint Stiffness, Particularly in the Morning
It may take 30 minutes or more before joints "loosen up."
Grating Sensation or Bone Spurs
A grinding feeling can occur as bone rubs against bone due to lost cartilage.
How a Pain Management Doctor Can Help Your Osteoarthritis:
Managing osteoarthritis means improving function and reducing inflammation without excessive reliance on medications. We may use image-guided joint injections, bracing, and regenerative treatments. Pain doctors also help patients adapt with assistive devices and lifestyle modifications.
Common treatments include:
Corticosteroid or hyaluronic acid joint injections
Physical and occupational therapy
Anti-inflammatory medications
Assistive supports like canes or orthotics
3. Chronic Neck Pain and Cervical Radiculopathy
Often caused by cervical disc herniation or arthritis that compresses spinal nerves. Poor posture, especially with prolonged screen time, is a growing cause in younger adults.
Symptoms of Chronic Neck Pain and Cervical Radiculopathy:
Localized Neck Pain
This may feel like soreness or burning pain that worsens with movement.
Radiating Pain Down the Arms
Indicates nerve root irritation in the cervical spine.
Numbness or Tingling in the Hands or Fingers
This is a sign of nerve compression or inflammation.
Muscle Weakness
You may have difficulty gripping objects or experience arm fatigue.
Headaches Originating From the Neck
Tension and nerve irritation can cause referred pain into the skull.
How a Pain Management Doctor Can Help :
Our team focuses on identifying the source of the nerve compression. We use imaging-guided cervical injections, therapeutic exercises, and posture correction strategies. Nerve blocks or ablation may be used for stubborn pain.
Possible interventions include:
Cervical epidural steroid injections
Neuromuscular re-education
Postural therapy
Targeted pain medications
4. Chronic Pain from Sciatica
Sciatica is caused by irritation of the sciatic nerve which can often be caused by a herniated disc or bone spur. Spinal stenosis or pelvic trauma may also contribute.
Symptoms of Chronic Pain from Sciatica:
Shooting Pain From the Lower Back Down One Leg
Often described as electric or burning, it can worsen with prolonged sitting.
Burning or Tingling Sensations
Typically felt along the sciatic nerve path.
Weakness in the Leg or Foot
May affect balance, walking, or climbing stairs.
Pain That Worsens When Sitting or Standing for Long Periods
Certain positions increase pressure on the nerve root.
Difficulty Walking
Pain may become sharp or radiate with movement.
How a Pain Management Doctor Can Help:
Treatment focuses on reducing nerve inflammation and preventing flare-ups. POA specialists use targeted injections, movement re-education, and sometimes minimally invasive procedures to decompress the nerve.
Treatment strategies may include:
Lumbar epidural injections
Sciatic nerve blocks
Decompression exercises
Anti-neuropathic medications
5. Complex Regional Pain Syndrome (CRPS)
CRPS can develop after surgery, fracture, or sprain. It involves abnormal nerve responses and inflammation that affect the central nervous system's pain regulation.
Symptoms of CRPS:
Severe, Ongoing Pain in One Limb
Pain that is often disproportionate to what would be expected from the initial injury.
Swelling and Skin Color Changes
The limb may appear red, blue, or blotchy.
Sensitivity to Touch (Allodynia)
Even light brushing or temperature changes cause significant pain.
Decreased Mobility or Joint Stiffness
The affected area may become hard to move or hypersensitive.
Temperature or Sweating Irregularities
One limb may feel noticeably warmer or colder.
How a Pain Management Doctor Can Help:
CRPS is complex and requires early, aggressive treatment. Our physicians often use sympathetic nerve blocks, spinal cord stimulation, and desensitization therapy to restore mobility and decrease hypersensitivity.
Interventions may include:
Sympathetic nerve blocks
Spinal cord stimulation
Desensitization therapy
Multidisciplinary rehab
Other Common Chronic Pain Conditions
Fibromyalgia
A widespread chronic pain condition that affects muscles and soft tissues, often accompanied by fatigue, memory issues ("fibro fog"), and sleep disturbances.
Symptoms include:
Constant, dull body aches
Tender points across the body
Extreme fatigue and non-restorative sleep
Heightened sensitivity to pain and temperature
Chronic Headaches and Migraines
Recurring, often debilitating head pain that can last hours to days. Migraines that are frequently accompanied by nausea, light sensitivity, and aura.
Symptoms can include:
Experiencing throbbing or pulsing pain, typically on one side
Having sensitivity to light, sound, or smells
Feelings of nausea or vomiting
Having visual disturbances or aura (flashes, blind spots)
Pain stemming from wear and tear, inflammation, or stiffness of the shoulder joint or tendons. It can severely limit arm function.
Symptoms include:
Dull or sharp pain in the shoulder or upper arm
Stiffness or "locking" in the joint
Weakness with lifting or overhead movement
Difficulty sleeping on the affected side
Post-Surgical or Post-Traumatic Pain Syndromes
Pain that persists beyond normal healing after surgery or injury, often involving nerve damage or tissue hypersensitivity.
Symptoms include:
Persistent pain at the surgical or injury site
Burning, tingling, or stabbing sensations
Increased pain with touch or movement
Limited function in the affected area
Why See a POA Pain Management Specialist?
Seeing a pain management doctor at POA isn't just about getting medication or another procedure—it's about reclaiming your life. Our physicians take a whole-person approach to your care. That means listening closely, examining thoroughly, and crafting a treatment plan to meet your needs, lifestyle, and goals.
Whether your pain has lasted months or years, our team is equipped with the tools and experience to make a difference. We blend advanced medical technologies with human compassion. Our goal is to help you move better, sleep longer, work easier, and engage in life again—on your terms.
Pain doesn't need to define who you are or what you can do. With the right care, you can get your life back—and it starts with a conversation at POA.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
Living with a Herniated Disc: Understanding the Condition and Treating the Pain
You’re bending over to tie your shoe, or maybe you just lifted a laundry basket off the floor—and suddenly, something shifts. A sharp, electric jolt shoots through your lower back and radiates down your leg. Within days, sitting becomes excruciating. You feel tingling in your foot. Or worse—your leg feels weak, like it might buckle underneath you.
It's not just a sore back. You could be dealing with a herniated disc—a spine condition that can disrupt your daily life, mobility, and comfort. But the good news? It’s treatable, and in many cases, you can fully recover without surgery.
What Is a Herniated Disc (And Is It the Same as a Slipped Disc)?
Your spine is made up of 33 vertebrae, and between most of them are intervertebral discs—soft, cushion-like pads that absorb shock and allow flexibility in your back.
Each disc has two parts:
A soft, gel-like inner core (the nucleus pulposus)
A tough, fibrous outer shell (The annulus fibrosus)
A herniated disc, also known as a ruptured disc or colloquially as a “slipped disc”, occurs when the inner core pushes out through a crack or tear in the outer shell. This herniation can press against nearby nerves, triggering pain, numbness, tingling, or weakness—depending on the location and severity of the compression.
Slipped disc vs. herniated disc: While the term "slipped disc" is commonly used, nothing actually “slips” out of place. The disc material bulges or leaks, which is more accurately described as a herniation.
The Difference Between a Bulging Disc and a Herniated Disc
Herniated Disc
Bulging Disc
What it is
The disc's inner gel-like material breaks through a tear in the tough outer layer. The outer wall is torn or ruptured.
The disc extends outward beyond its normal boundary, usually evenly around the disc's circumference. The outer wall remains intact but stretched out.
Severity
Typically, more severe than a bulging disc. Especially if it compresses nearby nerves.
Often considered less severe than a herniated disc and can often be asymptomatic.
Symptoms
Sharp pain, sciatica, numbness, tingling, or weakness in the limbs.
Mild back pain or none at all. Sometimes asymptomatic.
Causes
Trauma, heavy lifting, or progression of a bulging disc.
Degeneration from aging, posture, and repetitive stress.
Treatment
May need physical therapy, injections, or even surgery if conservative care fails.
Often responds to conservative care and lifestyle changes.
Symptoms of a Herniated Disc
Symptoms of a herniated disc depend on the location of the herniation and which nerves are affected. In general, the most common areas are the lumbar (lower back) and cervical (neck) spine.
Lumbar Herniated Disc Symptoms:
Sharp or burning low back pain:
This may feel like a stabbing pain that worsens when you move, bend, or sit.
Sciatica:
Pain that radiates from your lower back into your buttocks and down one leg, sometimes reaching the foot.
Numbness or tingling in the legs or feet:
A “pins and needles” sensation along the path of the affected nerve.
Muscle weakness:
You may find it harder to lift your foot (foot drop), stand on your toes, or walk normally.
Pain that worsens with activity:
Especially while sitting, coughing, sneezing, or straining.
Cervical Herniated Disc Symptoms:
Neck pain:
Often persistent and sharp.
Radiating arm pain:
From the neck down into the shoulder, arm, and even into the hand.
Tingling or numbness in the fingers:
Often felt in specific fingers depending on the affected nerve root.
Arm weakness:
Difficulty gripping or lifting objects.
Do Herniated Discs Heal on Their Own?
In many cases, herniated discs heal without surgical intervention. Your body has the ability to reabsorb the protruding disc material and reduce inflammation around the affected nerve.
How Long Does It Take to Heal?
The recovery timeline depends on the severity of the herniation and the treatment used. It can take time and varies depending on your health, age, and activity level:
Severity
Differentiator
Recovery Timeframe
Mild-Moderate
Responds to rest, physical therapy, and medication.
4-6 weeks
Persistent
Involves nerve compression or recurrent flare-ups.
8-12+ weeks
Chronic or Severe
Presents with significant neurological symptoms.
Extensive treatment or surgical intervention
What Causes a Herniated Disc?
The most common causes of a herniated disc can include:
Age-related disc degeneration: As we get older, discs lose hydration and elasticity, making them more prone to tearing.
Repetitive stress or motion: Frequent bending, lifting, or twisting can wear down the outer disc layers.
Sudden trauma: Car accidents, sports injuries, or heavy lifting with improper form can cause acute disc rupture.
Poor posture and sedentary lifestyle: Slouching and weak core muscles put extra stress on the spine.
Obesity: Extra weight increases pressure on spinal discs.
Smoking: Reduces oxygen supply to spinal tissues and accelerates disc degeneration.
What Should You Do Immediately If You Suspect a Herniated Disc?
If you experience sudden back or neck pain along with radiating symptoms, take the following steps:
Stop any strenuous activity: Avoid lifting, twisting, or bending.
Apply cold packs (for the first 48 hours): Reduces inflammation and pain.
Switch to heat after 2–3 days: Relaxes tight muscles and improves circulation.
Over-the-counter medications: NSAIDs (like ibuprofen) help reduce swelling and pain.
Stay mobile—lightly: Short walks are better than prolonged bed rest, which can weaken muscles and delay healing.
Track your symptoms: Take note of any numbness, tingling, or weakness.
Meet Our Orthopaedic Spine Specialists
Seeing a Doctor for a Herniated Disc
When Should You See an Orthopaedic Specialist?
If you suspect you have a herniated disc, don’t wait. If you have any of the following symptoms you should seek care as soon as possible:
Pain that doesn’t improve after a week of rest and home care
Numbness or tingling that spreads or worsens
Muscle weakness, especially in your legs or arms
Trouble with your balance or coordination
Loss of bladder or bowel control (this is a medical emergency called cauda equina syndrome)
What Kind of Specialist Should You See?
For the best outcomes, consult with an orthopaedic specialist. At POA, these may include:
Orthopaedic Spine Surgeons: Our orthopaedic surgeons who are experts in surgical and nonsurgical care of spinal disorders.
Physical Medicine & Rehabilitation Physicians: Thes physicians focus on conservative and physical rehabilitation approaches.
Pain Management Specialists: If more agressive care is not neede our spesialists may offer injections, nerve blocks, or other targeted treatments.
Every person is unique so every treatment approach and plan is tailored for your specific needs.
How Is a Herniated Disc Diagnosed?
A typical diagnosis can include a review of your medical history such as prior injuries, sumptom patterns, lifestyle, and your work habits. It also involves a physical exam which may include reflex testing, muscle strength, raings of motion, and nerve response.
Imaging may also be ordered to assist in a comprehensive evaulation.
Imaging to evaluate a herniated disc may include:
MRI (Magnetic Resonance Imaging): Shows disc herniation and nerve impingement in detail
CT Scan (Computed Tomography): Offers detailed bone and disc imaging
X-rays: Useful to rule out fractures or arthritis but won’t show disc herniation directly
EMG (Electromyography): Measures how well nerves and muscles function and detects damage
Treatment For Herniated Disc
Conservative (Non-Surgical) Treatments:
Physical Therapy: Core strengthening, stretching, and posture correction exercises to relieve pressure on the affected nerve.
Medications:
NSAIDs (ibuprofen, naproxen) for pain and inflammation
Muscle relaxants for spasms
Nerve pain medications (gabapentin or pregabalin)
Activity Modification: Limiting activities that aggravate symptoms while staying gently active.
Epidural Steroid Injections: Reduce inflammation around the nerve root and provide temporary relief.
Minimally Invasive Surgical Options(if conservative care fails):
Microdiscectomy: This is where a small portion of the disc is removed to free the compressed nerve.
Endoscopic Discectomy: Performed through a thin tube using a camera, often with quicker recovery.
Extensive Surgical Options(for severe cases):
Laminectomy: Removes part of the vertebra to relieve pressure on nerves.
Spinal Fusion: Joins two or more vertebrae together to stabilize the spine when discs are severely damaged.
Why Choose a POA Spine Specialist?
At POA, we specialize in restoring comfort, strength, and movement—without rushing to surgery.
What sets us apart:
✅ Board-certified spine specialists with years of experience in both conservative and advanced surgical care.
✅ Personalized treatment plans: Tailored to your body, lifestyle, and goals.
✅ Commitment to conservative care first: We explore every non-surgical option before recommending surgery.
✅ Multidisciplinary approach: Orthopaedic surgeons, physical therapists, and pain specialists collaborate on your care.
✅ Advanced diagnostics: Immediate access to imaging and nerve studies for fast, accurate diagnosis
Whether you’re newly injured or have struggled with back pain for months, POA’s spine experts can help you get your life back on track.
You Deserve to Feel Better
A herniated disc can feel like a life-altering injury, but it doesn’t have to be. With the right care team and a focused treatment plan, recovery is not only possible—it’s probable. Don’t wait in pain! Schedule with one of our Orthopaedic Spine Specialists today and take your first step toward relief and recovery.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
Living with Plantar Fasciitis
You know the pain well. As you rise from bed every morning, you place your feet on the floor, only to be greeted with a sharp, stabbing sensation in your heel. It's like a jolt that reminds you that the pain isn't gone yet. After walking around for a few minutes, the discomfort may ease. Still, it always comes back when you've been on your feet too long, especially after resting or sleeping. This is a daily struggle for those living with plantar fasciitis – a condition that affects your ability to walk comfortably and can take a toll on your overall quality of life.
What is Plantar Fasciitis?
Plantar fasciitis occurs when a thick connective tissue running from your heel to your toes along the bottom of your foot (plantar fascia) becomes irritated and inflamed. The plantar fascia supports the foot's arch and is essential for proper foot movement and support while walking. Excessive strain or overstretching can cause tiny tears in the fascia, triggering inflammation and discomfort, particularly in the heel.
While plantar fasciitis is frequently seen in physically active individuals, it can affect anyone. Symptoms tend to worsen in the morning when the tissue tightens during sleep, causing significant discomfort with the day's first steps.
Who Gets Plantar Fasciitis?
If you’ve ever felt a sharp, stabbing pain in your heel when you step out of bed in the morning, you may be dealing with plantar fasciitis—one of the most common causes of heel pain. This condition affects millions of people each year, but it’s not random. Certain groups are more likely to develop it based on lifestyle, footwear choices, and physical activity.
1. Runners and Athletes
People who run regularly or participate in high-impact sports are among the most common groups to experience plantar fasciitis symptoms. Repetitive motion, especially without proper stretching or supportive footwear, can cause microtears in the plantar fascia. Increasing mileage too quickly, running on hard surfaces, or using worn-out shoes can all contribute to heel pain in runners.
2. People Who Stand All Day
Working a job that keeps you on your feet for hours at a time can put you more at risk for developing plantar fasciitis. Teachers, nurses, warehouse workers, and retail staff often experience chronic foot and heel pain due to the constant pressure on their feet—especially if they’re standing on hard surfaces like concrete or not wearing cushioned shoes.
3. Those with Excess Body Weight
Carrying extra weight puts more pressure on your feet and heels, making it harder for your plantar fascia to do its job. This is especially true during long periods of walking or standing. Losing even a modest amount of weight can often reduce pain and prevent further damage.
4. People with Foot Structure or Gait Issues
Your natural foot shape or the way you walk could be behind your chronic heel pain. People with flat feet, high arches, or those who overpronate (roll their feet inward too much) often experience more strain on the plantar fascia, leading to irritation and inflammation. Tight calf muscles or a limited range of motion in your Achilles tendon can also increase your risk.
5. Adults Between Ages 40–60
Unfortunately, age is another common factor. Middle-aged adults are more likely to develop plantar fasciitis due to natural wear and tear. The connective tissue in our bodies loses elasticity as we age, making us more prone to injury from overuse or poor support.
6. People Who Wear Unsupportive Shoes
Let’s talk about your footwear! Flip-flops, ballet flats, high heels, and worn-out sneakers all share the same issue, they offer little to no arch support. Wearing these types of shoes regularly can increase your risk of developing plantar fasciitis, especially if you're walking long distances or spending hours on your feet.
Why you can trust us:
We have multiple highly specialized, board-certified, fellowship-trained orthopaedic surgeons.
We know that we serve people - actual humans - not random orthopaedic conditions. That drives us to compassionate care.
The world of orthpaedics is constantly evolving. Our orthopaedic surgeons are constantly evaluating new techniques, tools and methods to serve our community even better.
We provide outcome-focused treatment. We work with our patients to achieve their goals, all while developing custom treatment plans that fit our patient's lives.
The symptoms of plantar fasciitis can vary in intensity but generally include:
Heel pain – The most common symptom is a sharp pain, often felt in the center or at the bottom of the heel. It can feel like a stabbing sensation, making walking difficult, especially after resting.
Pain after rest – The pain is typically more severe after long periods of sitting or lying down, such as when you first get out of bed or after long periods of inactivity.
Swelling: Mild swelling may occur at the bottom of the heel, especially after standing for extended periods.
Pain with prolonged standing or walking may decrease as you walk. Still, after prolonged periods of standing or after physical activity, the pain can return and become more intense.
Stiffness – After sitting or lying down for a long time, the bottom of the foot can feel stiff, making it difficult to take the first few steps of the day.
Causes of Plantar Fasciitis
Several contributing factors can lead to plantar fasciitis. Understanding these causes of plantar fasciitis can help prevent the condition or reduce the risk of recurrence:
Overuse and repetitive stress
Plantar fasciitis is often caused by repetitive activity that stresses the plantar fascia. High-impact activities like running or jumping can overstrain this tissue, especially if done incorrectly or without proper footwear.
Improper footwear
Shoes that lack adequate arch support, cushioning or are worn-out can exacerbate heel pressure. High heels, flip-flops, or shoes with flat soles may contribute to this strain.
Foot structure abnormalities
People with flat feet, high arches, or abnormal gait patterns may place excessive stress on the plantar fascia. The added strain causes the tissue to become overstretched, leading to inflammation and pain.
Obesity or excess weight
Extra weight puts additional pressure on the feet, making them more susceptible to injury and strain. Over time, this additional weight can cause microtears in the plantar fascia, leading to plantar fasciitis.
Tight calf muscles or Achilles
Having tightness in the calves or Achilles tendon can affect how pressure distributes across your feet. This adds stress to the plantar fascia, increasing the likelihood of inflammation and discomfort.
Aging
As you age, the plantar fascia loses some elasticity and shock-absorbing properties. This makes the tissue more prone to tears and inflammation, leading to plantar fasciitis, especially in people over 40.
When to See an Orthopedic Specialist For Plantar Fasciitis
You can usually manage plantar fasciitis with at-home treatments. Still, sometimes, certain situations warrant a visit to an orthopedic specialist.
Signs to see an orthopaedic specialist for plantar fasciitis:
Persistent pain – If your plantar fasciitis pain lasts more than a few weeks despite your self-care efforts, it's time to seek professional help. Chronic pain could mean the inflammation has not subsided and may require more aggressive treatment.
Difficulty walking – If the pain interferes with your ability to walk or complete daily tasks, seeking care from an orthopedic specialist is essential.
No improvement with over-the-counter treatments – If over-the-counter pain relievers or home remedies like ice and stretching haven't brought any relief, you might need more specialized care to resolve the issue.
Swelling and bruising – If you experience swelling, bruising, or warmth around the heel, it could signal more than just plantar fasciitis. An orthopedic specialist will perform diagnostic tests to ensure no other underlying injury.
Nerve damage symptoms – If you experience numbness, tingling, or weakness in your foot, this could be a sign of nerve involvement, which requires immediate attention.
How to Treat Plantar Fasciitis at Home
Here are several strategies you can use at home to help relieve the pain and inflammation associated with plantar fasciitis:
Rest and avoid high-impact activities
Giving your foot time to heal is essential. Avoid activities that involve running, jumping, or standing for long periods, as these can further irritate the plantar fascia.
Ice therapy
Applying an ice pack to your heel for 15-20 minutes several times throughout the day can help reduce inflammation and pain.
OTC anti-inflammatory medications
Medications like ibuprofen or naproxen can reduce inflammation and relieve pain. Be sure to follow the recommended dosage and consult a doctor if needed.
Stretching exercises
Stretching your calf muscles, Achilles tendon, and the plantar fascia can help alleviate your pain and prevent stiffness. Simple exercises like towel stretches or calf stretches can improve your flexibility and reduce the strain on your foot.
Foot supports
Wearing supportive shoes with proper arch support and cushioning can reduce pressure on your plantar fascia. Orthotic insoles may also help distribute pressure more evenly across your foot.
Night splints
Wearing night splints can help maintain a light stretch of the plantar fascia while you sleep. This helps prevent the fascia from tightening during the night and reduces morning pain.
How to Prevent Plantar Fasciitis
Preventing plantar fasciitis is possible but it involves making adjustments to your daily habits and lifestyle.
How to prevent plantar fasciitis:
Wear proper footwear – Select footwear that provides the right arch support, cushioning, and stability for your heels. Avoid walking barefoot on hard surfaces and limit prolonged use of high heels to reduce strain on your feet.
Regular Stretching – Regularly stretch your calves, Achilles tendons, and feet to improve flexibility and reduce the risk of strain on the plantar fascia.
Maintain a healthy weight – Keeping your weight within a healthy range will help to reduce the strain on your feet, decreasing your chances of developing plantar fasciitis.
Take breaksto rest – If you stand or walk for long periods, take breaks to rest your feet and alleviate pressure. If you can't take breaks, alternating between sitting and standing can also help prevent overuse.
Strengthen your feet and lower legs – Exercises that strengthen your calf muscles, foot muscles, and ankle stabilizers can help prevent plantar fasciitis by improving foot mechanics and reducing excessive strain.
Exercises to Help Release and Heal Plantar Fasciitis
Here are some targeted exercises to help with plantar fasciitis:
Towel Stretch – Sitting on the floor with your legs stretched out in front of you, wrap a towel around the ball of your foot. Gently pull your foot toward you, feeling a stretch along the bottom of your foot and the back of your leg.
Calf Stretch – Stand arm's length facing a wall and step back with one leg. Keep your back leg straight and your heel planted on the ground. Place your hands on the wall at the height of your shoulders and lean forward, stretching your calf and Achilles tendon of your back leg.
Foot Roll – To help massage the plantar fascia and relieve built-up tension, you can use a tennis ball or similar ball under the arch of your foot. Once you place it, slowly roll it back and forth.
Toe Stretch – While sitting with your legs extended, reach for your toes and gently pull them toward your body. This stretch helps loosen the plantar fascia and should be held for 15-30 seconds before repeating.
Heel Raises – Stand with the balls of your feet on the edge of a step. Slowly lift yourself onto your toes, then lower your heels past the level of the step to stretch your calves and the bottom of your feet.
Whether you're a runner, a retail worker, or someone who loves their flip-flops a little too much, plantar fasciitis can sneak up on you. Knowing your risk factors is half the battle. With the right footwear, regular stretching, and paying attention to heel pain symptoms, you can take steps (literally!) to protect your feet.
Plantar fasciitis doesn't have to be a permanent issue. You can effectively manage and treat this painful condition with proper care, early intervention, and lifestyle adjustments. If your at-home treatments aren't bringing you relief or if your symptoms are worsening, Princeton Orthopaedic Associates is here to help. Our team of specialists can provide targeted therapies, advanced treatments, and personalized care to help you get back on your feet and live pain-free.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
Could Your Neck Pain Be a Pinched Nerve in the Neck?
You wake up with a stiff neck, thinking you just slept in an odd position. But as the day goes on, the pain doesn't go away. Instead, it radiates down your shoulder and into your arm. Simple tasks like turning your head, reaching for your phone, or even sitting at your desk become uncomfortable. You think, maybe you just slept weird and it will feel better tomorrow, except the pain doesn't improve, it continues for days, even weeks. This is what living with a pinched nerve in the neck can feel like—persistent discomfort that affects your daily life.
What is a Pinched Nerve in the Neck?
A pinched nerve in the neck, also known as cervical radiculopathy, occurs when excessive pressure is applied to a nerve root in the cervical spine (neck area). This pressure can come from surrounding structures such as bones, cartilage, muscles, tendons, or swollen tissues, leading to nerve irritation or compression. This compression disrupts the nerve's normal function and can lead to pain, tingling, weakness, or numbness in your neck.
Symptoms of a Pinched Nerve in the Neck
The symptoms you experience from a pinched nerve in the neck can vary from person to person, but generally speaking, the most common symptoms often involve a discomfort that radiates beyond your neck. You may experience a sharp or burning pain that extends into the shoulder, arm, or even down to the fingers, sometimes worsening with certain movements or prolonged positions. With the pain, there may be an unusual tingling or buzzing sensation, almost like the affected area has "fallen asleep," which can become persistent or intermittent. You may also notice weakness in their grip or find it harder to perform tasks requiring fine motor skills, as the nerve's ability to send signals to the muscles is compromised. In more severe cases, prolonged compression can lead to a feeling of numbness or loss of sensation in certain areas, making it difficult to tell if you're touching something or feeling temperature changes properly.
Symptoms of a pinched nerve in the neck:
Pain in your neck: Sharp, aching, or burning pain localized in the neck area.
Radiating pain or discomfort extending from your neck to your shoulder, arm, or even fingers.
Limited range of motion – Difficulty turning your head or tilting your neck without pain.
Numbness or tingling: A sensation of reduced or lost feeling in the affected area, sometimes accompanied by a "pins and needles" or prickling feeling.
Muscle weakness – Difficulty lifting objects or performing everyday tasks due to weakened muscles.
Why you can trust us:
We have multiple highly specialized, board-certified, fellowship-trained orthopaedic surgeons.
We know that we serve people - actual humans - not random orthopaedic conditions. That drives us to compassionate care.
The world of orthpaedics is constantly evolving. Our orthopaedic surgeons are constantly evaluating new techniques, tools and methods to serve our community even better.
We provide outcome-focused treatment. We work with our patients to achieve their goals, all while developing custom treatment plans that fit our patient's lives.
The causes of a pinched nerve in the neck can vary from person to person, but generally speaking, they stem from excessive pressure or irritation affecting the nerves in your spine in the neck. In many cases, age-related changes in the spine, such as degenerating discs or bone spurs, gradually narrow the space where nerves exit, leading to compression. Injuries, like sudden whiplash from a car accident or repetitive strain from poor posture, can also cause misalignments or inflammation that presses on the nerve. For some people, long hours spent looking down at a phone or sitting at a desk with improper ergonomics contribute to chronic strain, gradually leading to nerve irritation. Inflammatory conditions, like arthritis, or acute issues, such as a herniated disc leaking fluid onto nearby nerves, can also increase pressure, intensifying symptoms over time.
Causes of a pinched nerve in the neck:
Poor posture – Slouching or looking down at screens for long periods strains your neck.
Herniated disc – When the soft inner material of a spinal disc pushes through its outer layer. When doing so, it can create pressure on nearby nerves, leading to pain and discomfort.
Bone spurs – Overgrowth of bone in your spine can narrow the spaces where nerves travel.
Arthritis – Inflammation and degeneration of joints can lead to nerve compression.
Injury – Sudden impacts from accidents or sports can lead to nerve irritation.
Repetitive motions – Constant strain from work or activities like texting or carrying heavy bags can contribute.
When to Seek Care from an Orthopedic Spine Specialist
Pain persists for several weeks despite home treatments.
Weakness in your arms or hands affects daily tasks.
Loss of coordination or balance signals nerve damage beyond just discomfort.
Symptoms worsen over time, even with rest and self-care.
Loss of bowel or bladder control can sometimes happen and may indicate a more serious spinal condition requiring immediate attention.
How to Treat a Pinched Nerve in the Neck at Home
A pinched nerve can cause discomfort ranging from mild tingling to sharp, radiating pain that disrupts daily life. Whether it’s in your neck, back, or another area, this condition occurs when surrounding tissues—such as muscles, tendons, or bones—put excess pressure on a nerve. While severe cases may require medical attention, many pinched nerves can be relieved at home with simple, effective treatments.
From gentle stretches and posture adjustments to anti-inflammatory remedies and nerve-soothing techniques, here’s how you can ease pain and support your body’s natural healing process:
Rest and avoid aggravating movements – Rest is always important when it comes to home treatment. Try to minimize activities that strain your neck. Continued stress can worsen your inflammation and lengthen the time it takes for you to heal. Resting allows the affected nerve to recover without further irritation.
Apply heat or ice – Applying an ice pack to your neck within the first 48 hours of injury can help reduce swelling and numb pain. After the initial inflammation subsides, switching to a heating pad or warm compress can help improve blood circulation and relax tense muscles around the nerve.
Use over-the-counter pain relievers – Medications such as ibuprofen or naproxen can help alleviate pain and reduce inflammation, making it easier to perform daily tasks while healing.
Adjust your sleeping position – Sleeping with a supportive pillow, one that keeps your neck aligned with your spine, can relieve pressure on your pinched nerve. Sleeping on your back or side rather than your stomach is also beneficial to avoid excessive neck strain.
Gentle stretching – Performing slow and controlled neck stretches can help release the pinched nerve and improve mobility. Simple exercises such as chin tucks, neck tilts, and shoulder rolls can gradually reduce tension and enhance flexibility.
Maintain good posture – Practicing proper posture while sitting, standing, and using electronic devices can prevent further nerve compression. Keeping your shoulders back and your head aligned with your spine can significantly reduce neck strain.
Massage therapy – Massaging your neck and shoulder muscles can help improve circulation, reduce muscle tension, and promote relaxation.
Meet Our Orthopaedic Spine Specialists
How to Prevent a Pinched Nerve in the Neck
Preventing a pinched nerve in the neck starts with maintaining good posture, keeping muscles strong and flexible, and avoiding repetitive strain. Poor posture, prolonged screen time, and sleeping in awkward positions can all contribute to nerve compression, leading to pain, stiffness, and discomfort. By making small adjustments—such as improving ergonomics, incorporating regular stretching, and strengthening the neck and shoulders—you can reduce the risk of nerve irritation and keep your neck healthy and pain-free.
Here’s how to take proactive steps to prevent a pinched nerve before it starts.
Practice good posture – Keeping your head aligned with your spine reduces unnecessary strain on your neck. When working at a desk, ensure your monitor is at eye level, and your shoulders remain relaxed.
Take breaks from screens – Looking down at your phone or computer screen for long periods stresses your cervical spine. Taking frequent breaks, using a stand for devices, and adjusting screen height can help minimize the risk of nerve compression.
Strengthen your neck and shoulder muscles – Strengthening exercises such as chin tucks, shoulder blade squeezes, and resistance training can provide better support for your neck, reducing the likelihood of nerves becoming pinched.
Use proper ergonomics – Adjusting your workstation to include a supportive chair, a desk at the correct height, and a keyboard to encourage natural wrist alignment can prevent awkward neck positions contributing to nerve compression.
Avoid carrying heavy bags on one side – Carrying a heavy purse, backpack, or briefcase on one shoulder creates an imbalance that strains your neck muscles. Opt for a backpack with even weight distribution or frequently switch sides to help reduce stress on your cervical spine.
Sleep with proper support – Choosing a pillow that maintains the natural alignment of your neck and adopting a sleep position that keeps your spine in a neutral posture can help reduce strain and prevent excessive pressure on cervical nerves.
Maintain an active lifestyle – Regular exercise promotes flexibility, strengthens muscles, and improves overall spinal health, reducing the risk of nerve compression over time.
Exercises to Help Release and Heal a Pinched Nerve
When dealing with a pinched nerve, gentle movement and stretching can help alleviate pressure, improve mobility, and promote healing.
Below is a more detailed explanation of how to perform each exercise effectively:
1. Chin Tucks
Purpose: Strengthens the deep neck flexors, improves posture, and reduces strain on the cervical spine.
How to Do It:
Sit or stand with your spine straight.
Gently pull your chin straight back (as if making a double chin), keeping your head level.
Hold for 5-10 seconds, then relax.
Repeat 8-10 times.
Tip: Avoid tilting your head up or down—think of sliding your head straight back.
2. Neck Side Bends (Lateral Flexion Stretch)
Purpose: Stretches the muscles along the sides of your neck to reduce tension.
How to Do It:
Sit or stand with your shoulders relaxed.
Slowly tilt your head to one side, bringing your ear toward your shoulder.
Hold for 15-30 seconds, feeling the stretch along the opposite side of your neck.
Switch sides and repeat 3-5 times per side.
Tip: Keep your shoulders down and relaxed to get the full benefit of the stretch.
3. Neck Rotations
Purpose: Increases flexibility and reduces stiffness in the neck.
How to Do It:
Sit or stand with a straight back.
Slowly turn your head to the right, trying to look over your shoulder.
Hold for 5-10 seconds, then return to the center.
Repeat on the left side.
Do this 5-8 times on each side.
Tip: Move slowly and avoid forcing the stretch. If you feel pain, stop immediately.
4. Shoulder Rolls
Purpose: Relieves tension in the shoulders and neck, improving blood flow.
How to Do It:
Sit or stand with your arms relaxed at your sides.
Roll your shoulders forward in a circular motion 10 times.
Reverse the motion and roll them backward 10 times.
Tip: Perform this exercise slowly and deliberately, focusing on releasing tension in your upper back and neck.
5. Upper Trapezius Stretch
Purpose: Helps release tightness in the upper shoulders and neck, which can contribute to nerve compression.
How to Do It:
Sit or stand with a straight posture.
Tilt your head toward one shoulder.
Use your hand on the same side to apply light pressure, gently deepening the stretch.
Hold for 15-30 seconds, then switch sides.
Repeat 3-5 times per side.
Tip: Keep your opposite shoulder relaxed and down to maximize the stretch.
Final Tips:
Perform these exercises gently—never force a stretch.
Consistency is key; do them daily for best results.
If you experience sharp pain or worsening symptoms, stop immediately and consult a healthcare provider.
A pinched nerve in your neck can make daily activities difficult, but you don't have to live with chronic pain. You can find relief and restore normal function with proper care, treatment, and lifestyle adjustments. Our spine specialists here at Princeton Orthopaedics Associates are here to help if your symptoms persist or worsen. Reach out today for expert care and personalized treatment options to get you back to living pain-free.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.