We get it. We like our acronyms! Orthopaedic Surgeons, and doctors in general, often go around saying groups of letters as if everyone is going to get it.
That’s why we’ve created a comprehensive list to serve as a clear and reliable reference for our patients. Whether you’re reviewing test results, discussing a diagnosis with your physician, or reading about your recovery plan, this list can help you make sense of the medical language being used. Our goal is to empower patients with knowledge so that every conversation about your health is less intimidating and more productive.
Acronym
Full Title
Description
MD
Doctor of Medicine
Completed allopathic medical training. Focuses on traditional biomedical model and is licensed for full scope medical and surgical practice.
DO
Doctor of Osteopathic Medicine
Completes the same training as MDs with added emphasis on holistic care and musculoskeletal system. Licensed for full medical and surgical practice in the U.S.
PA-C
Physician Assistant, Certified
Graduate-level provider trained in diagnosis, treatment, and minor surgery. Works under physician supervision but can prescribe and manage care.
NP
Nurse Practitioner
Advanced practice registered nurse with graduate-level training. Provides diagnosis, treatment, and prescribing, often with a holistic emphasis.
DNP
Doctor of Nursing Practice
Highest clinical nursing degree with focus on evidence-based practice and leadership. Functions as an NP but with expanded academic and clinical training.
CRNA
Certified Registered Nurse Anesthetist
Advanced practice nurse specializing in anesthesia. Provides anesthesia independently or alongside anesthesiologists in surgery and trauma settings.
Bone & Joint Conditions
BMD – Bone Mineral Density: Measurement of bone strength using imaging (DEXA scan). Helps diagnose osteoporosis and fracture risk. Essential for long-term bone health monitoring.
CTS – Carpal Tunnel Syndrome: Compression of the median nerve at the wrist. Causes numbness, tingling, and hand weakness. Often treated with splints, injections, or surgery.
OA – Osteoarthritis: Degenerative joint disease due to cartilage breakdown. Causes pain, stiffness, and reduced range of motion. Common in hips, knees, and hands.
RSI – Repetitive Strain Injury: Overuse injury to muscles, tendons, or nerves. Common in wrists, elbows, and shoulders. Preventable with ergonomic adjustments.
Fractures & Fixation
FNF – Femoral Neck Fracture: Break in the neck of the femur, common in elderly after falls. High risk of complications due to disrupted blood supply. Treated with screws, arthroplasty, or hemiarthroplasty.
Fx / Frx – Fracture: Break in a bone. Classified by pattern, location, and stability. May require casting, fixation, or surgery.
DHS – Dynamic Hip Screw: Implant system for stabilizing femoral neck or intertrochanteric fractures. Allows controlled compression during healing. Inserted surgically into the femur.
SHS – Sliding Hip Screw: Similar to DHS, used for hip fracture stabilization. Provides controlled movement as the fracture heals. Widely used in orthopaedic trauma.
IMN – Intramedullary Nail: Rod placed inside bone marrow canal for fracture stabilization. Common in long bone fractures. Provides strong internal fixation.
CMN – Cephalomedullary Nail: Type of intramedullary nail extending into the femoral head. Stabilizes proximal femur fractures. Often chosen for unstable hip fractures.
ORIF – Open Reduction Internal Fixation: Surgical repair of fractures using plates, screws, or rods. “Open reduction” means exposing the bone surgically. “Internal fixation” stabilizes it from inside.
Ex-fix – External Fixator: Frame with pins/wires inserted into bone through skin. Stabilizes fractures or corrects deformities externally. Used in severe trauma or infection cases.
Arthroplasty & Joint Replacement
THA – Total Hip Arthroplasty: Complete hip replacement with artificial components. Relieves pain from arthritis or fractures. Improves mobility and quality of life.
TKA – Total Knee Arthroplasty: Replacement of the knee joint with artificial implants. Used for end-stage arthritis or deformity. Restores function and reduces pain.
TSA – Total Shoulder Arthroplasty: Replacement of the shoulder joint with prosthesis. Improves motion and relieves pain. Used for arthritis or severe fractures.
RSA – Reverse Shoulder Arthroplasty: Shoulder replacement where ball and socket are reversed. Provides stability when rotator cuff is deficient. Useful in complex shoulder conditions.
DFR – Distal Femoral Replacement: Prosthetic replacement of lower femur. Used in severe fractures or tumors. Restores knee joint stability and function.
Neuro & Physical Exam Terms
DTR – Deep Tendon Reflexes: Involuntary muscle contractions when tendon is tapped. Used to assess nerve and spinal cord function. Commonly tested in knees and ankles.
SILT – Sensation Intact to Light Touch: Exam finding documenting preserved skin sensation. Indicates intact nerve function. Common in trauma assessments.
AIN – Anterior Interosseous Nerve: Branch of the median nerve controlling thumb/index finger flexion. Injury causes weakness in pinch grip. Tested with “OK sign.”
PIN – Posterior Interosseous Nerve: Branch of the radial nerve controlling finger extension. Injury causes finger drop. Often injured in forearm trauma.
Motion & Weight Bearing
FROM – Full Range of Motion: Joint can move normally in all planes. Indicates absence of stiffness or contracture. Often documented in rehab notes.
PROM – Passive Range of Motion: Movement performed by examiner without patient effort. Tests joint flexibility and stiffness. Important in rehab and post-op recovery.
AROM – Active Range of Motion: Movement performed by patient voluntarily. Assesses muscle strength and function. Limited in cases of weakness or pain.
NWB – Non-Weight Bearing: Patient must not put weight on injured limb. Requires crutches, walker, or wheelchair. Standard after major fractures or surgery.
PWB – Partial Weight Bearing: Patient may put limited weight on limb. Usually specified as percentage (e.g., 25%). Step-down progression in rehab.
TTWB – Toe Touch Weight Bearing: Only toes lightly touch the ground for balance. No real weight through limb. Transition stage before partial weight bearing.
FFWB – Foot Flat Weight Bearing: Patient may rest entire foot but not load limb. Intermediate between TTWB and PWB. Used for gradual progression.
WBAT – Weight Bearing as Tolerated: Patient bears as much weight as comfortable. Limited only by pain. Common after stable fracture fixation.
Trauma & Mechanism
APC – Anterior Posterior Compression: Pelvic fracture pattern from front-to-back force. Causes pelvic instability and bleeding risk. Often from high-energy trauma.
LC – Lateral Compression: Pelvic fracture pattern from side-to-side force. Stability varies with severity. Common in vehicle or crush injuries.
GLF – Ground-Level Fall: Fall from standing height. Common cause of hip and wrist fractures in elderly. Often signals osteoporosis or frailty.
GSW – Gunshot Wound: Penetrating trauma from firearm. May involve bone, nerves, and vessels. Requires multidisciplinary care.
Materials
Provider & Professional Acronyms
Physicians
MD – Doctor of Medicine: Completed allopathic medical training. Focuses on traditional biomedical model. Trained in surgery, prescribing, and full scope practice.
DO – Doctor of Osteopathic Medicine: Completes same training as MD with additional focus on holistic care and musculoskeletal system. Uses osteopathic manipulative treatment (OMT). Licensed for full practice in the U.S.
Additional Physician Types
PA-C – Physician Assistant, Certified: Graduate-level medical provider trained in diagnosis, treatment, and minor surgery. Works under physician supervision. Can prescribe medication.
NP – Nurse Practitioner: Advanced practice registered nurse with graduate-level training. Provides diagnosis, treatment, and prescribing. Often emphasizes preventive and holistic care.
DNP – Doctor of Nursing Practice: Highest clinical degree for nursing. Focuses on leadership, evidence-based practice, and advanced clinical skills. Functions as an NP with expanded academic training.
Nursing & Allied Health
RN – Registered Nurse: Provides patient care, medication administration, and coordination. Licensed after nursing degree and national exam. Backbone of hospital and surgical teams.
LPN – Licensed Practical Nurse: Provides basic patient care under RN supervision. Training shorter than RN. Common in rehab and outpatient settings.
CNA – Certified Nursing Assistant: Assists patients with daily living tasks. Works under nurses’ supervision. Provides vital bedside support.
CRNA – Certified Registered Nurse Anesthetist: Advanced practice nurse specializing in anesthesia. Provides anesthesia independently or with anesthesiologists. Critical in surgery and trauma care.
Therapy & Rehabilitation
PT – Physical Therapist: Doctorate-level provider specializing in mobility, strength, and rehab. Designs exercise programs for recovery. Critical after surgery or injury.
DPT – Doctor of Physical Therapy: Doctoral degree in physical therapy (entry-level in U.S.). Focuses on evidence-based rehab care. Equivalent to PT but emphasizes doctoral training.
OT – Occupational Therapist: Helps patients regain independence in daily activities. Focuses on upper extremity function and adaptive strategies. Important post-surgery or after injury.
COTA – Certified Occupational Therapy Assistant: Works under OT supervision. Delivers therapy exercises and training. Provides hands-on patient support.
ATC – Athletic Trainer, Certified: Specializes in sports medicine, injury prevention, and rehab. Works with athletes and orthopaedic teams. Provides on-field and clinical support.
Surgical & Training Roles
FA – First Assistant: Assists primary surgeon with exposure, suturing, and technical tasks. Can be physician, PA, or NP. Enhances operative efficiency.
SA – Surgical Assistant: Supports surgeon intraoperatively with retraction, suction, and prep. May be trained staff or non-physician. Distinct from scrub nurse.
PGY-# – Post-Graduate Year: Indicates level of residency training. Example: PGY-3 = third-year resident. Determines experience and role in surgery.
MS4 – Fourth-Year Medical Student: Final year before graduation from medical school. May assist in surgery under supervision. Limited responsibilities compared to residents.
Certifications
FAAOS – Fellow of the American Academy of Orthopaedic Surgeons: Prestigious membership after board certification in orthopaedics. Indicates commitment to education and peer standards. Recognized globally in orthopaedics.
FACS – Fellow of the American College of Surgeons: Designation for surgeons meeting rigorous professional standards. Shows commitment to ethical and skilled surgical practice. Used across multiple specialties.
Why Does My Knee Pop? Common Causes and When to Get Help
Learn why knees sometimes pop, when it’s usually harmless, and when it may signal a problem. Common causes include gas bubbles or tendons snapping, but popping can also point to joint issues. Explore simple at-home steps that may help, and know when it’s time to see a clinician.
If you hear occasional popping without pain, it is usually not serious. But if popping comes with pain, swelling, instability, or locking, you should seek evaluation so we can find the cause and plan treatment.
Quick Overview: What This Post Covers
What makes knees pop.
How to tell harmless popping from trouble.
Simple self-care and when to see a specialist.
Tests and treatments your clinician may use.
How we approach diagnosis and recovery at Princeton Orthopaedic Associates.
Common, Usually Harmless Causes of Knee Popping
Sometimes popping is simply noise from normal joint movement. A few common benign reasons include:
Gas bubbles forming and popping inside the joint fluid, which can create a cracking sound
Tendons or ligaments snapping briefly as they shift over bone when the joint moves
Rough surfaces rubbing in a joint with age-related wear; osteoarthritis can also have inflammatory flares and management depends on symptoms and function
Painless popping alone is not known to cause arthritis; however, if popping is accompanied by pain, swelling, instability, or limits on function, you should have it evaluated.
When Popping May Mean a Problem
Popping that comes with other symptoms may point to an underlying injury. Watch for these signs:
Sharp or persistent pain at the time of popping
Visible swelling or the knee feeling hot
A feeling that the knee gives way, locks, or will not fully bend or straighten
Pain or instability that limits walking or daily activities
Those symptoms suggest we should examine the joint to look for cartilage injuries, meniscal tears, ligament strain, loose fragments, or significant joint inflammation.
Emergency or Urgent Signs
If any of the following occur after a pop, get urgent or emergency care rather than waiting for a routine appointment:
A loud pop during an injury followed by immediate swelling and inability to bear weight
Visible deformity or suspected patellar dislocation
The knee is locked and you cannot fully straighten it - true mechanical locking
Severe pain after trauma or when a fracture is suspected
A hot, very painful swollen knee with fever or chills, or a swollen painful knee in someone who is immunocompromised - possible septic arthritis
What Might Be Causing Painful Popping?
Several common issues can cause painful popping. These include damage to soft tissues, cartilage problems, and mechanical irritation around the joint.
Meniscal tears. A torn meniscus can catch or lock and may produce a pop with pain.
Ligament sprains. A sudden twist or direct blow can cause ligament stretching and an audible pop.
Patellar tracking issues and patellar instability or dislocation. If the kneecap moves unevenly or subluxes, you may feel or hear snapping and experience pain.
Loose bodies or osteochondral injury. Cartilage or bone fragments can catch in the joint and cause painful popping or locking.
Cartilage wear. As cartilage thins with age or injury, joint surfaces can make noise and become painful.
How We Evaluate Popping Knees
Your clinician will take a careful history and perform a focused exam to check motion, stability, and areas of tenderness. That helps narrow down likely causes.
Imaging and tests are selected based on the history and exam. X-rays are often first-line after trauma to assess for fracture and alignment; X-rays do not show soft tissues. MRI is ordered when the exam or history suggest soft tissue injury such as meniscus or ligament tears, cartilage damage, or when mechanical symptoms persist. Ultrasound can be useful for dynamic snapping and for evaluating superficial tendon or bursal problems.
Test
What it shows
X-ray
Bone alignment, fracture, and evidence of arthritis; does not show soft tissues
MRI
Soft tissues like meniscus, ligaments, and cartilage; used when exam or history suggest soft tissue injury or persistent mechanical symptoms
Ultrasound
Tendon or bursa irritation near the knee and useful for dynamic snapping
At-home Steps You Can Try First
If popping is mild and not accompanied by the concerning signs above, try conservative care while watching symptoms. Small changes often help.
Rest from the activity that triggers the sound for a few days
Ice the area for 10 to 15 minutes if there is pain or swelling
Over-the-counter nonsteroidal anti-inflammatory drugs may reduce pain; avoid NSAIDs if you have a history of gastrointestinal ulcers or bleeding, kidney disease, are taking blood thinners, are in late pregnancy, or have an NSAID allergy. If NSAIDs are not appropriate, consider acetaminophen after checking with your provider
Start gentle strengthening and mobility work for hips, quads, and hamstrings; a physical therapist can guide this
When You Should Schedule an Exam
Contact us for an evaluation if you have persistent pain, swelling, catching or locking, repeated giving way, or if symptoms prevent daily tasks. Early assessment helps us treat the cause and reduce the chance of longer term issues.
Who to See at Princeton Orthopaedic Associates
Specialty
Why you would see them
Sports Medicine
Non surgical evaluation for tendon, ligament, and meniscal problems
Orthopaedic Surgeon
Persistent mechanical symptoms or when surgery may be needed
Physical Therapist
Rehabilitation to improve strength, control, and movement patterns
What to Expect from Treatment
Treatment depends on the diagnosis. Many causes improve with a planned rehab program that reduces pain, restores motion, and strengthens supporting muscles. When structural damage is severe, surgical options may be discussed.
Conservative care first: activity modification, medication, targeted therapy
Procedures: injections may help for persistent inflammation
Surgery: reserved for clear mechanical problems or unresolving structural injury
If you want to discuss symptoms, we make it easy to schedule an exam. A focused visit helps us determine what is normal and what needs treatment so you can get back to your routine with confidence.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
That Aching or Sharp Pain in Your Shin Might Be Shin Splints
Whether you’re just trying to stay active, chasing after your kids, or if it's your teen pushing through practices and games, shin splints can stop you in your tracks. That aching, sometimes sharp pain along the front of the leg isn’t only for athletes running marathons, it’s surprisingly common in everyday life. Kids in fall sports like soccer, football, and cross-country often run into it, but parents and adults who spend long hours on their feet or squeeze in workouts can feel it too. What starts as a dull soreness after activity can quickly turn into a daily frustration, making simple things like walking, climbing stairs, or enjoying playtime harder than they should be. Shin splints don’t just interrupt sports; they interrupt life. This post explains what causes shin splints, how they feel, how we diagnose them, and practical steps you can take to feel better. We cover common triggers, home care, when to see a specialist, and what recovery usually looks like.
What this article will help you understand
You’ll learn why shin splints happen, what symptoms to watch for, which everyday habits make them worse, and how we at Princeton Orthopaedic Associates approach treatment and recovery.
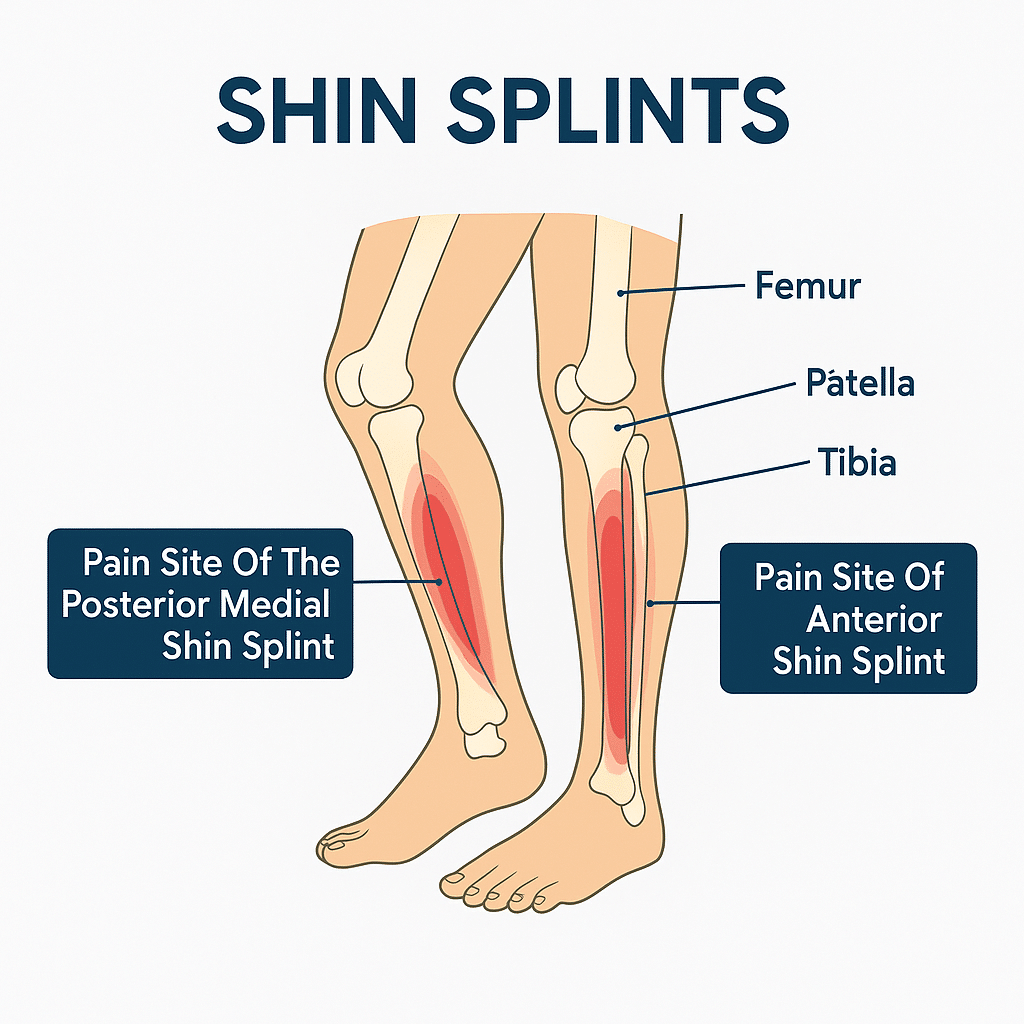
What Are Shin Splints?
Shin splints is a common name for pain along the shin bone that starts with activity. Classic shin splints most commonly refer to medial tibial stress syndrome, or MTSS, which presents as a diffuse aching along the posteromedial, or inner, border of the lower tibia near the distal half of the shin. Persistent pain over the front of the shin is less typical for MTSS and may indicate a tibial stress fracture or exertional compartment syndrome, so those symptoms should be evaluated.
MTSS is not just simple surface inflammation. It sits on a bone stress continuum where repeated overload affects the tibial cortex and the periosteum, and traction from muscles such as the soleus and tibialis posterior contributes to symptoms. We keep explanations simple but want you to know the pain often reflects mechanical overload of bone and the tissues attached to it.
How Shin Splints Typically Feel
Symptoms of shin splints usually start as a dull, aching pain along the inner edge of the lower leg, often felt during activity and easing with rest early on. The pain typically covers a broader segment along the posteromedial tibia rather than a single sharp spot.
Tenderness when you press along the shin, usually over a longer segment along the inner border
A dull, aching pain during or after exercise that may improve with rest at first
Visible swelling is uncommon in shin splints; marked swelling should prompt evaluation for other causes
Pain that gets worse if activity continues without change
By contrast, a tibial stress fracture more often causes focal point tenderness, a small spot that is exquisitely painful to press. Exertional compartment syndrome may produce tightness, cramping, numbness, or weakness during activity. If your pain is sharp, highly localized, wakes you at night, or makes it hard to walk, see a clinician promptly to check for these possibilities.
Common Causes and Who’s at Risk
Shin splints come from repetitive stress on the lower leg. You don’t have to be a runner to get them; they happen with many forms of exercise and work that increase load on the shin.
Sudden increases in training distance, speed, or duration
Starting a new activity without gradually building up
Running on hard or uneven surfaces
Worn or unsupportive shoes
Flat feet, high arches, or poor foot mechanics
Tight calf muscles or weak muscles that stabilize the ankle and foot
How We Confirm the Diagnosis
Diagnosis starts with a careful history and a physical exam. We check the pattern of pain, how it changes with activity, and look at your foot and ankle mechanics. The exam helps distinguish shin splints from a focal stress fracture or from exertional compartment syndrome.
If needed, imaging can help rule out a stress fracture or other conditions when symptoms are severe, very focal, or not improving with appropriate rest. X-rays are often the first test but can be normal early on. If concern persists, an MRI is more sensitive and can confirm a bone stress injury.
Treatment You Can Start at Home
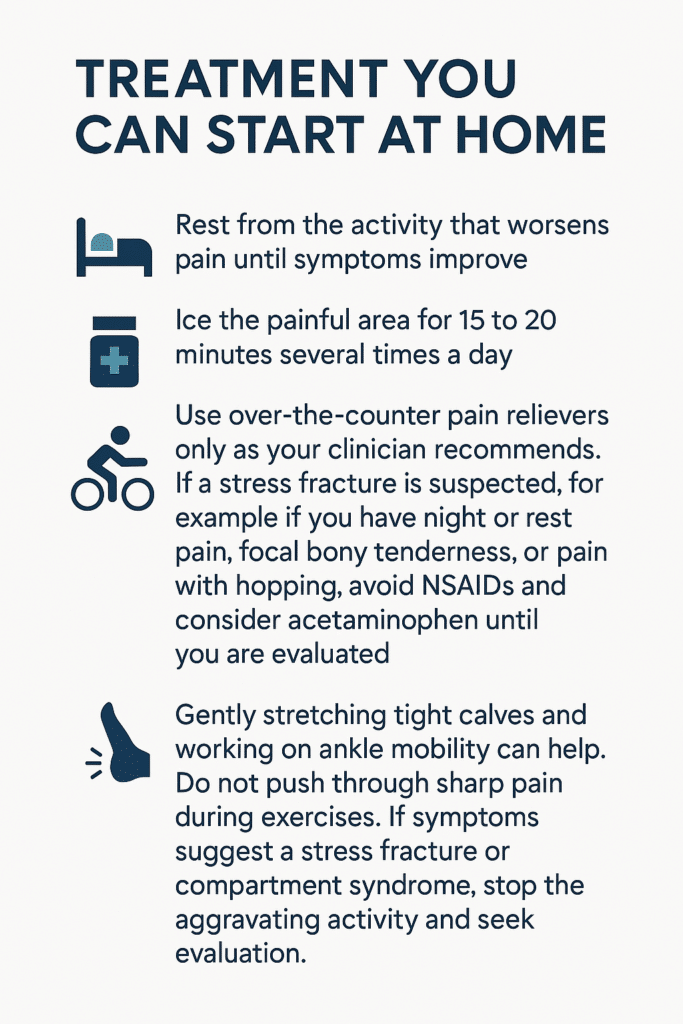
Rest from the activity that worsens pain until symptoms improve
Ice the painful area for 15 to 20 minutes several times a day
Use over-the-counter pain relievers only as your clinician recommends. If a stress fracture is suspected, for example if you have night or rest pain, focal bony tenderness, or pain with hopping, avoid NSAIDs and consider acetaminophen until you are evaluated
Try low-impact cross-training like swimming or cycling while you recover
Gently stretching tight calves and working on ankle mobility can help. Do not push through sharp pain during exercises. If symptoms suggest a stress fracture or compartment syndrome, stop the aggravating activity and seek evaluation.
Hands-on Care and Rehab
If symptoms persist, physical therapy is often the next step. A therapist will guide you through strengthening and flexibility work to correct the forces that stress the shin and help you return to activity safely.
Strengthening exercises for the calves, foot muscles, and hips
Progressive return-to-activity plans to avoid re-injury
Gait and footwear assessment, orthotics when appropriate
How Long Recovery Usually Takes
Recovery time varies based on severity and how quickly you address the cause. The table below gives a general idea.
Severity
Typical Recovery
Notes
Mild
2 to 4 weeks
Relative rest, icing, and gradual return usually helps.
Moderate
4 to 8 weeks
Often needs formal rehab and footwear changes.
Severe or Persistent
8 weeks or more
May require imaging and a structured rehab plan to avoid stress fracture risk.
Tips to Prevent Shin Pain from Returning
Increase training load slowly, by no more than 10 percent per week
Choose supportive shoes and replace them when they wear out
Add strength work for calves, hips, and foot muscles
Mix in low-impact cross-training to reduce repetitive stress
Run on softer surfaces when possible and avoid sudden downhill training
When You Should See a Provider
Seek care if pain is severe, gets worse despite rest, or you cannot put weight on the leg. Also see a clinician if pain wakes you at night, if you have marked swelling, or if you have new numbness or weakness.
Be alert for signs that need prompt or urgent evaluation, including:
Severe pain or inability to bear weight
Night pain or pain at rest that does not improve
Focal bony tenderness that is very painful to press, or pain with hopping, which may suggest a stress fracture
Escalating tightness in the lower leg during or after activity, new numbness or tingling, increasing weakness, foot drop, or pain that is out of proportion to the findings and does not settle with rest, which could indicate compartment syndrome
Worsening symptoms despite rest and conservative care
When foot mechanics, orthotics, or surgical options are considered
Helpful if foot structure contributes to repeat problems
Getting Back to Activity Safely
Return to activity should be gradual and guided by pain. Increase load slowly and stop if symptoms flare. A simple progression to consider is pain-free walking, then a pain-free single-leg hop, then light jogging. If those steps are comfortable, gradually increase duration and intensity while continuing strengthening and mobility work.
If you are unsure whether your pain is caused by shin splints or something more serious, schedule an exam so we can check you and recommend the right next steps.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
Pain On the Outside of Your Knee Could be IT Band Syndrome.
You don’t have to be a marathon runner to feel that nagging ache on the outside of your knee. The important thing? It might not actually be your knee. It might be a tight IT band, and unlike joint injuries, it requires a different kind of treatment focused on mobility and muscle balance.
Maybe it starts during your daily walk, or when you’re going up stairs. Perhaps it flares up when you get up from your desk or out of the car. It might even wake you up at night, pulsing in your outer thigh or hip, making it impossible to get comfortable. It doesn’t feel like an injury yet, the pain keeps coming back.
If this sounds familiar, there’s a good chance your iliotibial band (IT band) is involved. And the condition you might be dealing with is called IT Band Syndrome, a common cause of outer knee and hip pain that affects far more than just athletes.
Let’s walk through what’s happening in your body, why it hurts, and most importantly, what you can do to start feeling better.
Here Are The Things You Need to Know About IT Band Syndrome
What You Should Know:
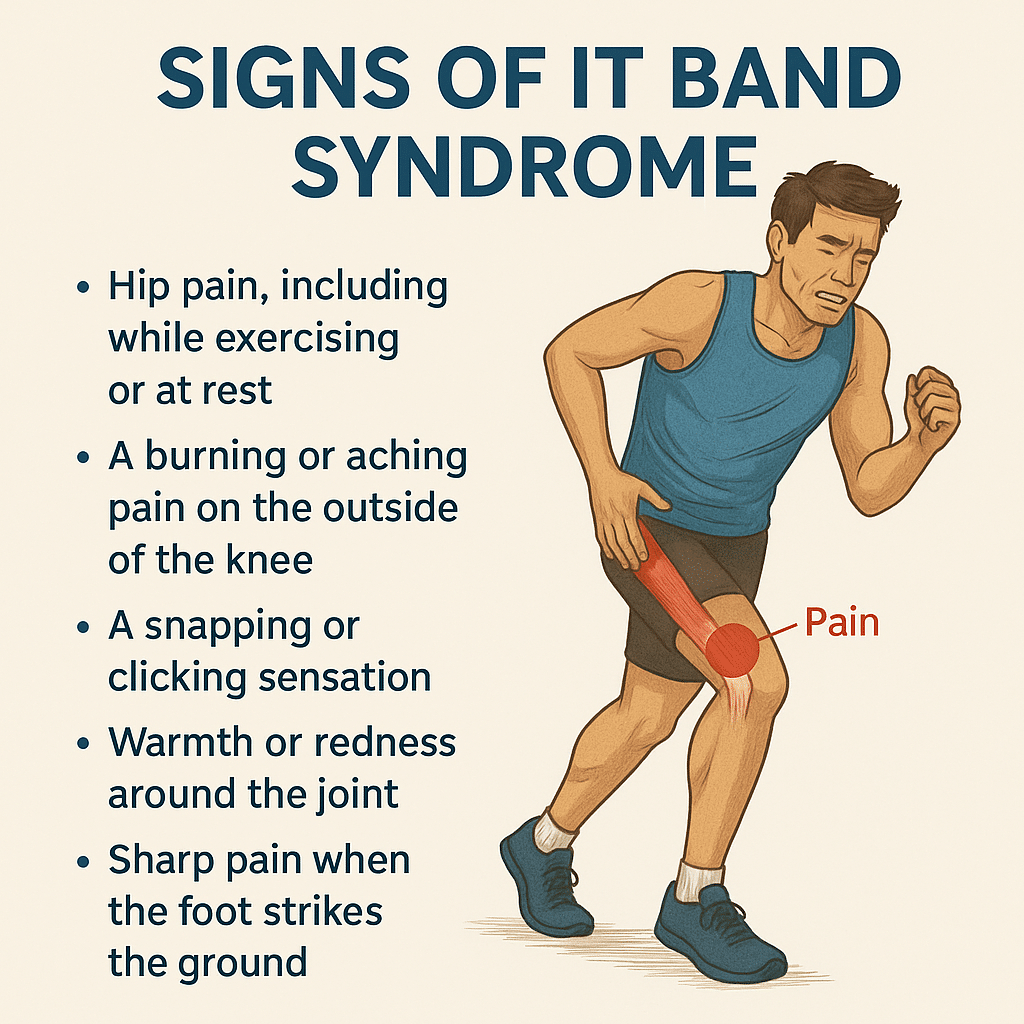
Pain on the outside of your knee or thigh is a common sign of IT Band Syndrome, and it's not just a runner's problem.
You don’t have to be an athlete. Everyday movement, prolonged sitting, or climbing stairs can all trigger symptoms.
The pain is caused by tightness and friction where the IT band rubs against bone near the knee.
Stretching the IT band itself won't solve the issue. Instead, focus on loosening surrounding muscles and improving strength.
Symptoms often show up with walking, going downstairs, or after long periods of inactivity.
The discomfort may travel up to your hip, outer thigh, or glute region, especially when lying on your side.
Causes often include weak glutes or core, poor posture, or worn-out shoes that don’t offer enough support.
Foam rolling can help, but you want to target the glutes, quads, and TFL, not directly on the IT band.
Recovery requires more than rest. Strengthening, mobility work, and correcting how you move are essential.
Seeing a physical therapist can help you address the root cause and get long-term relief.
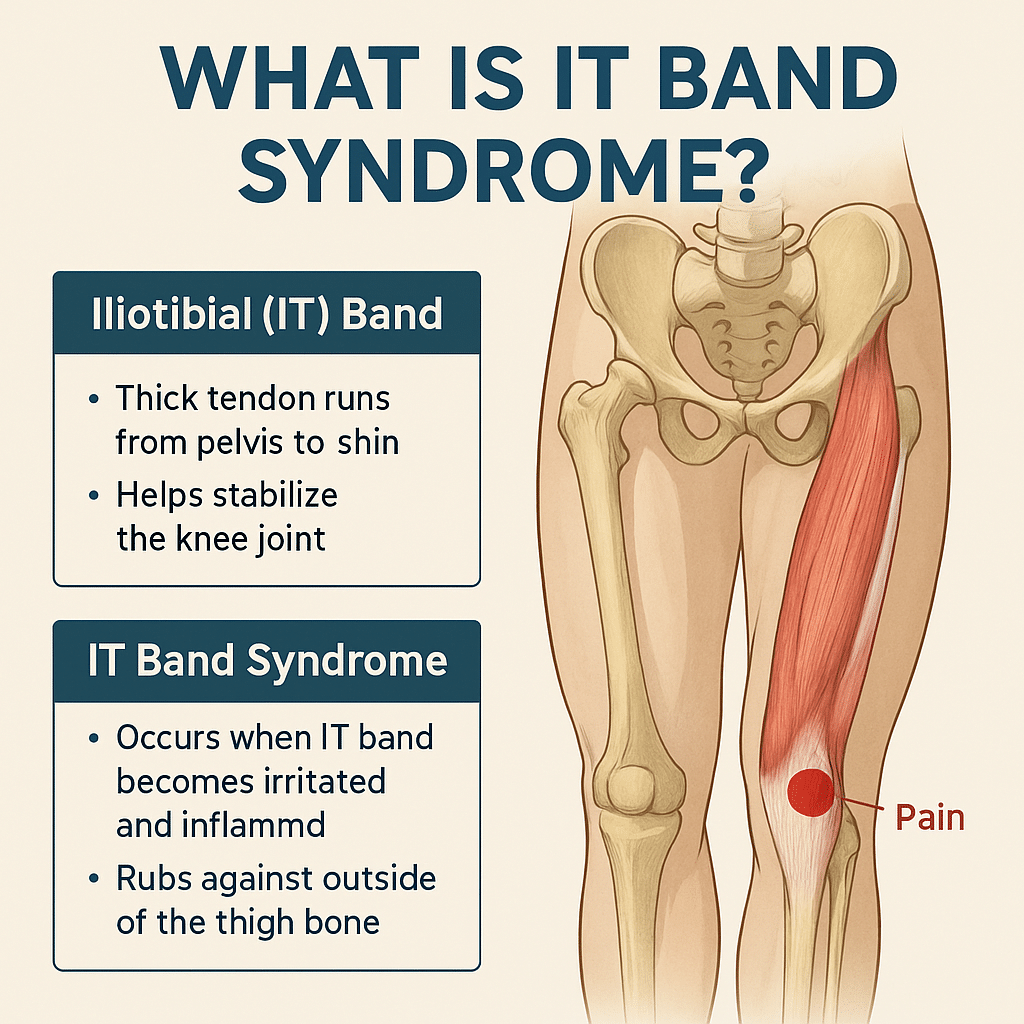
What Is the IT Band and Why Does It Get Tight?
The iliotibial (IT) band is a thick, fibrous band of connective tissue that runs down the outside of your leg, from your hip to just below your knee. Think of it as a support strap that helps stabilize your knee and assist with hip movement.
When the IT band gets too tight, often due to repetitive movement, muscle imbalances, or poor posture, it can rub against the bone at the outer knee. This creates irritation, inflammation, and pain, commonly known as IT Band Syndrome (ITBS).
And while it’s often associated with athletes, it’s just as common in walkers, desk workers, parents, nurses, retail workers, and anyone who’s on their feet a lot, or not enough.
What Does IT Band Syndrome Feel Like?
Here are common, real-world symptoms of IT Band Syndrome in everyday life:
Aching or burning pain on the outside of the knee
Tightness or pulling in the outer thigh
Pain or discomfort going up or down stairs
Sharp pain with walking or standing for extended periods
Tenderness at the hip or discomfort when lying on your side
Clicking or snapping near the hip or knee
These symptoms often start mild, but become more consistent if left unaddressed.
What Causes IT Band Syndrome in Non-Athletes?
Even without intense training, everyday habits can contribute to ITBS:
Sitting for long periods without movement
Poor posture or weak hip/core muscles
Uneven walking surfaces (like sloped sidewalks or hilly neighborhoods)
Wearing worn-out or unsupportive shoes
Standing or walking with one leg favored over the other
Repetitive daily movement without adequate strength or flexibility
What Causes IT Band Syndrome in Athletes?
While the core problem is the same (tightness and friction along the IT band), athletes often develop ITBS due to training volume and biomechanics. Common athletic triggers include:
Sudden increases in mileage or intensity (especially in runners and cyclists)
Downhill running or running on sloped surfaces
Repetitive activities involving knee flexion and extension
Weakness in hip abductors, glutes, or core stabilizers
Poor running form or gait asymmetries
Worn shoes or improper footwear for training conditions
Overtraining without proper rest and recovery
IT Band Syndrome is common among:
Distance runners
Cyclists
Soccer and hockey players
HIIT or CrossFit athletes
Skiers or hikers tackling long descents
💡 Tip for athletes:
Strengthen your hips and glutes, cross-train, and make sure your recovery matches your training load
.
Why Is IT Band Pain So Persistent?
The IT band isn’t a muscle, it’s actually connective tissue. That means:
You can’t stretch it the same way you stretch a muscle
If surrounding muscles (like glutes and hip flexors) are tight or weak, the IT band picks up the slack
Without correcting imbalances, foam rolling or resting alone won’t fix it
Over time, the friction and inflammation can become chronic and much harder to treat.
How Is IT Band Syndrome Treated?
Treatment focuses on reducing inflammation, improving mobility, and correcting muscle imbalances.
✅ Pain Relief & Inflammation Control
Ice the outer knee or thigh for 15–20 minutes at a time
Use anti-inflammatory medication if recommended by your doctor
Strengthen glutes, hips, and core to support proper leg mechanics
Stretch hip flexors, quads, hamstrings, and TFL
Foam roll the surrounding muscle groups but not directly on the IT band
✅ Movement & Habit Adjustments
Improve running or lifting form through coaching or therapy
Modify walking and standing posture
Use ergonomic tools (e.g., standing desks, supportive chairs)
Wear supportive shoes or orthotics if needed
How Long Does IT Band Syndrome Take to Heal?
The length of time to recover from IT Band Syndrome depends on how long you've had symptoms and whether you're treating the root cause:
Severity
Recovery Time
Notes
Mild
2-3 Weeks
Rest and stretching may help quickly if caught early
Moderate
4-6 Weeks
Requires active rehab including movement correction
Chronic
2+ Months
Long-standing tightness or inflammation takes time to unwind
Everyday Life with IT Band Syndrome
IT Band Syndrome doesn't just show up during workouts; it can quietly interfere with our daily routine, mobility, and overall comfort. Without treatment, ITBS can impact your:
Ability to walk, climb stairs, or stand comfortably
Sleep (especially side-sleepers)
Workday (especially for those on their feet)
Confidence in movement and balance
Long-term joint health if compensatory patterns develop
And for athletes, it can put your training on pause or create a cycle of recurring injuries.
Should I See a Doctor for a Tight IT Band?
If you have been experiencing symptoms of IT Band Syndrome and you haven't found relief, you should consult with a specialist. Especially if:
The pain has lasted more than a week
You’ve tried rest but symptoms return
You’re changing how you move to avoid pain
You’re unable to stay active or complete daily tasks comfortably
At Princeton Orthopaedic Associates, we have physicians from multiple specialties that can help you get to the root of your tight IT band and help set you off on the path to recovery.
- A physical therapist is often the next step after diagnosis for hands-on treatment and long-term recovery.
Our specialists will identify the root cause of your tightness, guide you through targeted corrective exercises, and help you improve how you move—not just mask the symptoms.
Stop Living With IT Band Pain
Whether you're training for a race or just trying to get through the workday without pain, IT Band Syndrome can be disruptive, but it's absolutely treatable. The key isn’t just stretching or resting, it's understanding why the IT band is tight and retraining your body to move in a healthier, more balanced way.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
Tweaked your knee, but the pain isn't going away?
You were mid-pivot, chasing a ball or turning to grab something behind you, when a sharp pop hit your knee. Not loud, but distinct. You paused, unsure if it was serious. Maybe just a tweak, you thought. But within hours, the swelling crept in, the joint stiffened, and walking suddenly felt unfamiliar. That small twist? It turned into something much bigger.
That moment likely marked the beginning of a meniscus tear—a common yet disruptive injury affecting the cartilage in your knee. Whether it's from a sudden injury or years of wear and tear, the result is often the same: pain, limited movement, and questions about what comes next.
What Is a Meniscus Tear?
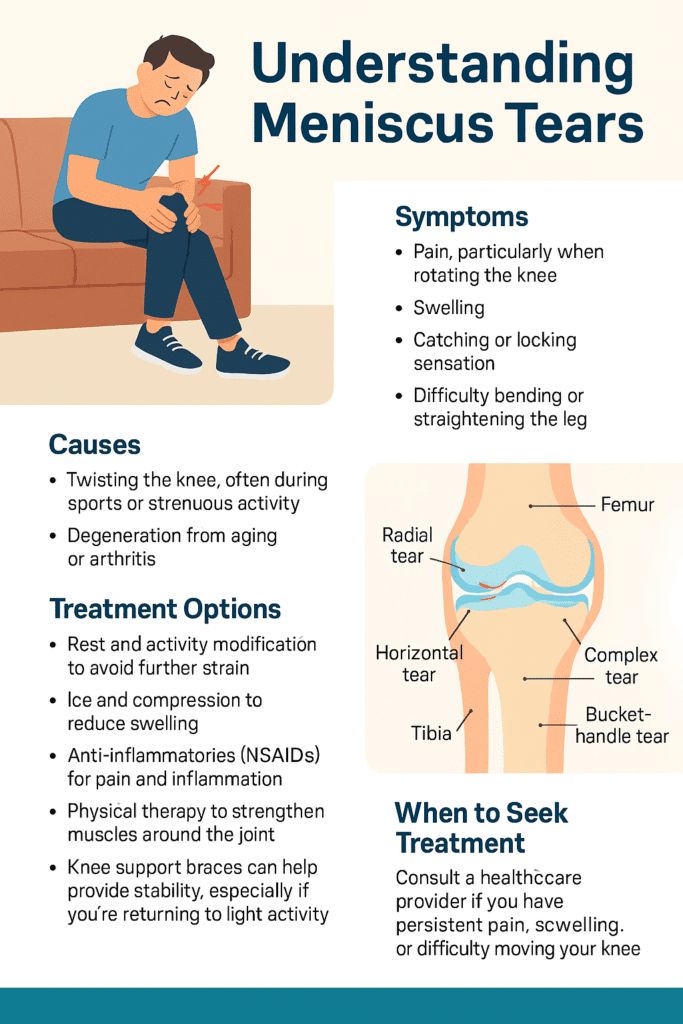
Inside each of your knees are two rubbery, wedge-shaped pieces of cartilage: the medial and lateral menisci. These act like shock absorbers between your thighbone and shinbone, helping to distribute weight and stabilize movement. A tear occurs when this cartilage is damaged—usually from twisting motions or degeneration over time.
You don't have to be an athlete for this to happen. A quick squat, an awkward turn, even standing up too fast with pressure on the joint can be enough, especially if the cartilage is already weakened with age.
Common Causes
There are two primary culprits behind a torn meniscus:
Trauma or sudden movement, like twisting or pivoting during sports, or while playing with your kids!
Degeneration, where age-related wear and tear thins and weakens the cartilage, making it easier to tear with minor movements.
Both scenarios are incredibly common. Lifting a heavy box incorrectly or kneeling on a hard surface for too long can be all it takes.
Meet Our Orthopaedic Knee Specialists
Symptoms of a Meniscus Tear
The first few hours after the tear are often the most telling. At first, discomfort may be the only symptom of a meniscus tear you might feel. Or, the only symptoms of a meniscus tear present at first are just a dull, persistent ache, made worse by movement. You might feel fine while sitting, but as soon as you try to walk or bend, your knee doesn't cooperate. Some describe it as a "stuck" sensation, where the joint feels like it won't fully extend or flex without pain or resistance. But then the pain deepens, swelling begins, and your range of motion shrinks even more.
Clicking, popping, or catching during movement can also indicate a torn flap of cartilage catching in the joint. Check out this post to read more about the Types of Meniscus Tears.
Additional Symptoms of a Meniscus Tear:
Locking, catching, or the feeling of instability
Sharp or aching pain, often on the inner (medial) side of the knee
Swelling that develops gradually
A popping sound or sensation during injury
Difficulty straightening or bending the knee
If you're looking for clarification on the symptoms of a meniscus tear, you are not alone. Many people deal with a torn meniscus and don't realize the seriousness until the stiffness and pain don't go away.
Do You Need to See a Doctor For a Meniscus Tear?
If you're hoping it will just go away, consider this: untreated meniscus tears can worsen over time, leading to more pain and even long-term joint issues like osteoarthritis.
Seek professional help if:
Pain persists beyond a few days
Swelling continues or worsens
You experience locking, buckling, or instability
You can't put normal weight on the leg
Ignoring it risks further tearing or cartilage breakdown. Early diagnosis often means better, less invasive treatment options.
Why you can trust us:
We have multiple highly specialized, board-certified, fellowship-trained orthopaedic surgeons.
We know that we serve people - actual humans - not random orthopaedic conditions. That drives us to compassionate care.
The world of orthpaedics is constantly evolving. Our orthopaedic surgeons are constantly evaluating new techniques, tools and methods to serve our community even better.
We provide outcome-focused treatment. We work with our patients to achieve their goals, all while developing custom treatment plans that fit our patient's lives.
A physical exam can often provide early clues. A clinician will test your range of motion and apply gentle pressure or rotation to identify pain points. In many cases, imaging, like an MRI, is used to confirm the diagnosis and pinpoint the severity and location of the tear.
Meniscus Tear Remedy
Not all meniscus tears require surgery. If you're looking for a meniscus tear remedy, treatment depends on the type of tear, location, and severity of the tear, as well as your activity level and age.
Conservative Meniscus Tear Remedy Approaches:
Rest and Activity Modification
One of the first things you can do is to give your knee a break! If you are able to identify them, avoid movements thatmake the pain worse. Common ones include twisting, squatting, or any high-impact activities. Resting allows the damaged cartilage in your knee to settle and inflammation to subside which gives your body a chance to begin healing. This doesn't mean you have to be totally immoble, but be mindful of your movements and eliminate anything that causes discomfort or strain.
Ice and Compression
Applying ice packs to your knee helps reduce swelling and numbs the area, easing the pain. Aim for 15–20 minutes every few hours in the first few days. Pair this with a compression bandage or sleeve to minimize inflammation and support the knee structure. Together, they help control the body's inflammatory response and provide short-term relief while preventing further irritation.
Anti-inflammatories (NSAIDs)
Over-the-counter medications like ibuprofen (Advil) or naproxen (Aleve) can significantly reduce inflammation and help manage pain. These drugs target the body’s natural inflammatory chemicals, making it easier to move the joint and complete daily activities without aggravating the tear. Always follow dosage instructions and consult your doctor if you’re taking them for more than a few days.
Physical Therapy
Once the pain and swelling are under control, targeted exercises become essential. A physical therapist will guide you through movements designed to strengthen the muscles surrounding your knee—especially the quadriceps and hamstrings. This not only speeds up recovery but also restores joint stability, improves flexibility, and reduces the risk of re-injury.
Knee Support Braces
A well-fitted knee brace offers additional stability, particularly when walking or performing light activities. Braces help limit unwanted lateral movement and protect the joint during recovery. If your knee tends to feel unstable or you're easing back into exercise or work, wearing a brace can provide the support and confidence you need to move safely.
Small tears near the outer edge, where the blood supply is richer, often heal with conservative care.
Surgical Options:
If the tear is large, causes locking, or doesn't improve, arthroscopic surgery may be recommended. Options include:
Meniscus repair (stitching the cartilage back together)
Partial meniscectomy (removing the torn section)
Total meniscectomy (rare and typically avoided)
Surgery is more likely in younger, active individuals or when the tear is in a critical area.
Torn Meniscus Recovery Timeline
How long it takes a torn meniscus to heal depends entirely on the treatment path and your consistency with rehab. Below is a general idea of recovery times based on the type of treatment - this is for reference only and not a diagnosis and treatment.
Treatment Method
Est. Recovery Time
Conservative (rest, PT)
4-8 weeks
Partial Meniscectomy
4-6 weeks
Arthroscopic Repair
3-6 months
So, how long does it take for a meniscus tear to heal? It may take time to regain strength and trust in your knee even after healing.
Meniscus Tear Common Questions
Can You Walk With a Meniscus Tear?
Yes—but that doesn't mean you should. Many people are able to walk with a torn meniscus, especially if the pain is mild. But without proper treatment, walking on a torn meniscus can cause further damage or transform a minor tear into a more serious one.
If you must stay mobile, supportive bracing and avoiding twisting motions is essential.
What Does a Torn Meniscus Look Like on The Outside
Despite the pain and swelling, a torn meniscus often doesn't present visible signs like bruising or discoloration. That's why if you're looking for answers to "what does a torn meniscus look like on the outside," the truth is, it doesn't look like much so you won't find much. The damage is internal; symptoms often show through movement limitations and experienced pain, not appearance.
How to Prevent a Meniscus Tear
Prevention of a meniscus tear isn't just about avoiding sports injuries—it's about daily movement, posture, and support.
Smart Prevention Strategies:
While it's no guarantee you'll avoid having a torn meniscus, there are some smart prevention strategies! Some strategies include:
Warm up: Before starting any physical activity, properly warm up to loosen up your muscles in preparation for the activity.
Stretch regularly: Regularly stretching, especially the hamstrings and calves, can also be helpful.
Strengthen: Doing strengthening work on leg muscles (quads, glutes, hamstrings) helps to improve stability. You'll want to avoid deep squats or twisting under load
Knee supports: If you know you're prone to injury or returning from one, wearing knee supports can be beneficial to prevent a meniscus tear.
You don't need to be an athlete to tear your meniscus—and you don't need to live with the pain either. Even activities like walking the dog or playing with your kids carry risk if you're not mindful of sudden directional changes! With awareness, early action, and proper care, recovery is possible and often complete. Pain-free movement starts with taking your symptoms seriously, getting the right diagnosis, and committing to healing fully.
If it feels wrong, it probably is. Trust your body, and give it what it needs to bounce back. Contact us today to schedule with one of our specialists.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
Living with a Herniated Disc: Understanding the Condition and Treating the Pain
You’re bending over to tie your shoe, or maybe you just lifted a laundry basket off the floor—and suddenly, something shifts. A sharp, electric jolt shoots through your lower back and radiates down your leg. Within days, sitting becomes excruciating. You feel tingling in your foot. Or worse—your leg feels weak, like it might buckle underneath you.
It's not just a sore back. You could be dealing with a herniated disc—a spine condition that can disrupt your daily life, mobility, and comfort. But the good news? It’s treatable, and in many cases, you can fully recover without surgery.
What Is a Herniated Disc (And Is It the Same as a Slipped Disc)?
Your spine is made up of 33 vertebrae, and between most of them are intervertebral discs—soft, cushion-like pads that absorb shock and allow flexibility in your back.
Each disc has two parts:
A soft, gel-like inner core (the nucleus pulposus)
A tough, fibrous outer shell (The annulus fibrosus)
A herniated disc, also known as a ruptured disc or colloquially as a “slipped disc”, occurs when the inner core pushes out through a crack or tear in the outer shell. This herniation can press against nearby nerves, triggering pain, numbness, tingling, or weakness—depending on the location and severity of the compression.
Slipped disc vs. herniated disc: While the term "slipped disc" is commonly used, nothing actually “slips” out of place. The disc material bulges or leaks, which is more accurately described as a herniation.
The Difference Between a Bulging Disc and a Herniated Disc
Herniated Disc
Bulging Disc
What it is
The disc's inner gel-like material breaks through a tear in the tough outer layer. The outer wall is torn or ruptured.
The disc extends outward beyond its normal boundary, usually evenly around the disc's circumference. The outer wall remains intact but stretched out.
Severity
Typically, more severe than a bulging disc. Especially if it compresses nearby nerves.
Often considered less severe than a herniated disc and can often be asymptomatic.
Symptoms
Sharp pain, sciatica, numbness, tingling, or weakness in the limbs.
Mild back pain or none at all. Sometimes asymptomatic.
Causes
Trauma, heavy lifting, or progression of a bulging disc.
Degeneration from aging, posture, and repetitive stress.
Treatment
May need physical therapy, injections, or even surgery if conservative care fails.
Often responds to conservative care and lifestyle changes.
Symptoms of a Herniated Disc
Symptoms of a herniated disc depend on the location of the herniation and which nerves are affected. In general, the most common areas are the lumbar (lower back) and cervical (neck) spine.
Lumbar Herniated Disc Symptoms:
Sharp or burning low back pain:
This may feel like a stabbing pain that worsens when you move, bend, or sit.
Sciatica:
Pain that radiates from your lower back into your buttocks and down one leg, sometimes reaching the foot.
Numbness or tingling in the legs or feet:
A “pins and needles” sensation along the path of the affected nerve.
Muscle weakness:
You may find it harder to lift your foot (foot drop), stand on your toes, or walk normally.
Pain that worsens with activity:
Especially while sitting, coughing, sneezing, or straining.
Cervical Herniated Disc Symptoms:
Neck pain:
Often persistent and sharp.
Radiating arm pain:
From the neck down into the shoulder, arm, and even into the hand.
Tingling or numbness in the fingers:
Often felt in specific fingers depending on the affected nerve root.
Arm weakness:
Difficulty gripping or lifting objects.
Do Herniated Discs Heal on Their Own?
In many cases, herniated discs heal without surgical intervention. Your body has the ability to reabsorb the protruding disc material and reduce inflammation around the affected nerve.
How Long Does It Take to Heal?
The recovery timeline depends on the severity of the herniation and the treatment used. It can take time and varies depending on your health, age, and activity level:
Severity
Differentiator
Recovery Timeframe
Mild-Moderate
Responds to rest, physical therapy, and medication.
4-6 weeks
Persistent
Involves nerve compression or recurrent flare-ups.
8-12+ weeks
Chronic or Severe
Presents with significant neurological symptoms.
Extensive treatment or surgical intervention
What Causes a Herniated Disc?
The most common causes of a herniated disc can include:
Age-related disc degeneration: As we get older, discs lose hydration and elasticity, making them more prone to tearing.
Repetitive stress or motion: Frequent bending, lifting, or twisting can wear down the outer disc layers.
Sudden trauma: Car accidents, sports injuries, or heavy lifting with improper form can cause acute disc rupture.
Poor posture and sedentary lifestyle: Slouching and weak core muscles put extra stress on the spine.
Obesity: Extra weight increases pressure on spinal discs.
Smoking: Reduces oxygen supply to spinal tissues and accelerates disc degeneration.
What Should You Do Immediately If You Suspect a Herniated Disc?
If you experience sudden back or neck pain along with radiating symptoms, take the following steps:
Stop any strenuous activity: Avoid lifting, twisting, or bending.
Apply cold packs (for the first 48 hours): Reduces inflammation and pain.
Switch to heat after 2–3 days: Relaxes tight muscles and improves circulation.
Over-the-counter medications: NSAIDs (like ibuprofen) help reduce swelling and pain.
Stay mobile—lightly: Short walks are better than prolonged bed rest, which can weaken muscles and delay healing.
Track your symptoms: Take note of any numbness, tingling, or weakness.
Meet Our Orthopaedic Spine Specialists
Seeing a Doctor for a Herniated Disc
When Should You See an Orthopaedic Specialist?
If you suspect you have a herniated disc, don’t wait. If you have any of the following symptoms you should seek care as soon as possible:
Pain that doesn’t improve after a week of rest and home care
Numbness or tingling that spreads or worsens
Muscle weakness, especially in your legs or arms
Trouble with your balance or coordination
Loss of bladder or bowel control (this is a medical emergency called cauda equina syndrome)
What Kind of Specialist Should You See?
For the best outcomes, consult with an orthopaedic specialist. At POA, these may include:
Orthopaedic Spine Surgeons: Our orthopaedic surgeons who are experts in surgical and nonsurgical care of spinal disorders.
Physical Medicine & Rehabilitation Physicians: Thes physicians focus on conservative and physical rehabilitation approaches.
Pain Management Specialists: If more agressive care is not neede our spesialists may offer injections, nerve blocks, or other targeted treatments.
Every person is unique so every treatment approach and plan is tailored for your specific needs.
How Is a Herniated Disc Diagnosed?
A typical diagnosis can include a review of your medical history such as prior injuries, sumptom patterns, lifestyle, and your work habits. It also involves a physical exam which may include reflex testing, muscle strength, raings of motion, and nerve response.
Imaging may also be ordered to assist in a comprehensive evaulation.
Imaging to evaluate a herniated disc may include:
MRI (Magnetic Resonance Imaging): Shows disc herniation and nerve impingement in detail
CT Scan (Computed Tomography): Offers detailed bone and disc imaging
X-rays: Useful to rule out fractures or arthritis but won’t show disc herniation directly
EMG (Electromyography): Measures how well nerves and muscles function and detects damage
Treatment For Herniated Disc
Conservative (Non-Surgical) Treatments:
Physical Therapy: Core strengthening, stretching, and posture correction exercises to relieve pressure on the affected nerve.
Medications:
NSAIDs (ibuprofen, naproxen) for pain and inflammation
Muscle relaxants for spasms
Nerve pain medications (gabapentin or pregabalin)
Activity Modification: Limiting activities that aggravate symptoms while staying gently active.
Epidural Steroid Injections: Reduce inflammation around the nerve root and provide temporary relief.
Minimally Invasive Surgical Options(if conservative care fails):
Microdiscectomy: This is where a small portion of the disc is removed to free the compressed nerve.
Endoscopic Discectomy: Performed through a thin tube using a camera, often with quicker recovery.
Extensive Surgical Options(for severe cases):
Laminectomy: Removes part of the vertebra to relieve pressure on nerves.
Spinal Fusion: Joins two or more vertebrae together to stabilize the spine when discs are severely damaged.
Why Choose a POA Spine Specialist?
At POA, we specialize in restoring comfort, strength, and movement—without rushing to surgery.
What sets us apart:
✅ Board-certified spine specialists with years of experience in both conservative and advanced surgical care.
✅ Personalized treatment plans: Tailored to your body, lifestyle, and goals.
✅ Commitment to conservative care first: We explore every non-surgical option before recommending surgery.
✅ Multidisciplinary approach: Orthopaedic surgeons, physical therapists, and pain specialists collaborate on your care.
✅ Advanced diagnostics: Immediate access to imaging and nerve studies for fast, accurate diagnosis
Whether you’re newly injured or have struggled with back pain for months, POA’s spine experts can help you get your life back on track.
You Deserve to Feel Better
A herniated disc can feel like a life-altering injury, but it doesn’t have to be. With the right care team and a focused treatment plan, recovery is not only possible—it’s probable. Don’t wait in pain! Schedule with one of our Orthopaedic Spine Specialists today and take your first step toward relief and recovery.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
Living with Plantar Fasciitis
You know the pain well. As you rise from bed every morning, you place your feet on the floor, only to be greeted with a sharp, stabbing sensation in your heel. It's like a jolt that reminds you that the pain isn't gone yet. After walking around for a few minutes, the discomfort may ease. Still, it always comes back when you've been on your feet too long, especially after resting or sleeping. This is a daily struggle for those living with plantar fasciitis – a condition that affects your ability to walk comfortably and can take a toll on your overall quality of life.
What is Plantar Fasciitis?
Plantar fasciitis occurs when a thick connective tissue running from your heel to your toes along the bottom of your foot (plantar fascia) becomes irritated and inflamed. The plantar fascia supports the foot's arch and is essential for proper foot movement and support while walking. Excessive strain or overstretching can cause tiny tears in the fascia, triggering inflammation and discomfort, particularly in the heel.
While plantar fasciitis is frequently seen in physically active individuals, it can affect anyone. Symptoms tend to worsen in the morning when the tissue tightens during sleep, causing significant discomfort with the day's first steps.
Who Gets Plantar Fasciitis?
If you’ve ever felt a sharp, stabbing pain in your heel when you step out of bed in the morning, you may be dealing with plantar fasciitis—one of the most common causes of heel pain. This condition affects millions of people each year, but it’s not random. Certain groups are more likely to develop it based on lifestyle, footwear choices, and physical activity.
1. Runners and Athletes
People who run regularly or participate in high-impact sports are among the most common groups to experience plantar fasciitis symptoms. Repetitive motion, especially without proper stretching or supportive footwear, can cause microtears in the plantar fascia. Increasing mileage too quickly, running on hard surfaces, or using worn-out shoes can all contribute to heel pain in runners.
2. People Who Stand All Day
Working a job that keeps you on your feet for hours at a time can put you more at risk for developing plantar fasciitis. Teachers, nurses, warehouse workers, and retail staff often experience chronic foot and heel pain due to the constant pressure on their feet—especially if they’re standing on hard surfaces like concrete or not wearing cushioned shoes.
3. Those with Excess Body Weight
Carrying extra weight puts more pressure on your feet and heels, making it harder for your plantar fascia to do its job. This is especially true during long periods of walking or standing. Losing even a modest amount of weight can often reduce pain and prevent further damage.
4. People with Foot Structure or Gait Issues
Your natural foot shape or the way you walk could be behind your chronic heel pain. People with flat feet, high arches, or those who overpronate (roll their feet inward too much) often experience more strain on the plantar fascia, leading to irritation and inflammation. Tight calf muscles or a limited range of motion in your Achilles tendon can also increase your risk.
5. Adults Between Ages 40–60
Unfortunately, age is another common factor. Middle-aged adults are more likely to develop plantar fasciitis due to natural wear and tear. The connective tissue in our bodies loses elasticity as we age, making us more prone to injury from overuse or poor support.
6. People Who Wear Unsupportive Shoes
Let’s talk about your footwear! Flip-flops, ballet flats, high heels, and worn-out sneakers all share the same issue, they offer little to no arch support. Wearing these types of shoes regularly can increase your risk of developing plantar fasciitis, especially if you're walking long distances or spending hours on your feet.
Why you can trust us:
We have multiple highly specialized, board-certified, fellowship-trained orthopaedic surgeons.
We know that we serve people - actual humans - not random orthopaedic conditions. That drives us to compassionate care.
The world of orthpaedics is constantly evolving. Our orthopaedic surgeons are constantly evaluating new techniques, tools and methods to serve our community even better.
We provide outcome-focused treatment. We work with our patients to achieve their goals, all while developing custom treatment plans that fit our patient's lives.
The symptoms of plantar fasciitis can vary in intensity but generally include:
Heel pain – The most common symptom is a sharp pain, often felt in the center or at the bottom of the heel. It can feel like a stabbing sensation, making walking difficult, especially after resting.
Pain after rest – The pain is typically more severe after long periods of sitting or lying down, such as when you first get out of bed or after long periods of inactivity.
Swelling: Mild swelling may occur at the bottom of the heel, especially after standing for extended periods.
Pain with prolonged standing or walking may decrease as you walk. Still, after prolonged periods of standing or after physical activity, the pain can return and become more intense.
Stiffness – After sitting or lying down for a long time, the bottom of the foot can feel stiff, making it difficult to take the first few steps of the day.
Causes of Plantar Fasciitis
Several contributing factors can lead to plantar fasciitis. Understanding these causes of plantar fasciitis can help prevent the condition or reduce the risk of recurrence:
Overuse and repetitive stress
Plantar fasciitis is often caused by repetitive activity that stresses the plantar fascia. High-impact activities like running or jumping can overstrain this tissue, especially if done incorrectly or without proper footwear.
Improper footwear
Shoes that lack adequate arch support, cushioning or are worn-out can exacerbate heel pressure. High heels, flip-flops, or shoes with flat soles may contribute to this strain.
Foot structure abnormalities
People with flat feet, high arches, or abnormal gait patterns may place excessive stress on the plantar fascia. The added strain causes the tissue to become overstretched, leading to inflammation and pain.
Obesity or excess weight
Extra weight puts additional pressure on the feet, making them more susceptible to injury and strain. Over time, this additional weight can cause microtears in the plantar fascia, leading to plantar fasciitis.
Tight calf muscles or Achilles
Having tightness in the calves or Achilles tendon can affect how pressure distributes across your feet. This adds stress to the plantar fascia, increasing the likelihood of inflammation and discomfort.
Aging
As you age, the plantar fascia loses some elasticity and shock-absorbing properties. This makes the tissue more prone to tears and inflammation, leading to plantar fasciitis, especially in people over 40.
When to See an Orthopedic Specialist For Plantar Fasciitis
You can usually manage plantar fasciitis with at-home treatments. Still, sometimes, certain situations warrant a visit to an orthopedic specialist.
Signs to see an orthopaedic specialist for plantar fasciitis:
Persistent pain – If your plantar fasciitis pain lasts more than a few weeks despite your self-care efforts, it's time to seek professional help. Chronic pain could mean the inflammation has not subsided and may require more aggressive treatment.
Difficulty walking – If the pain interferes with your ability to walk or complete daily tasks, seeking care from an orthopedic specialist is essential.
No improvement with over-the-counter treatments – If over-the-counter pain relievers or home remedies like ice and stretching haven't brought any relief, you might need more specialized care to resolve the issue.
Swelling and bruising – If you experience swelling, bruising, or warmth around the heel, it could signal more than just plantar fasciitis. An orthopedic specialist will perform diagnostic tests to ensure no other underlying injury.
Nerve damage symptoms – If you experience numbness, tingling, or weakness in your foot, this could be a sign of nerve involvement, which requires immediate attention.
How to Treat Plantar Fasciitis at Home
Here are several strategies you can use at home to help relieve the pain and inflammation associated with plantar fasciitis:
Rest and avoid high-impact activities
Giving your foot time to heal is essential. Avoid activities that involve running, jumping, or standing for long periods, as these can further irritate the plantar fascia.
Ice therapy
Applying an ice pack to your heel for 15-20 minutes several times throughout the day can help reduce inflammation and pain.
OTC anti-inflammatory medications
Medications like ibuprofen or naproxen can reduce inflammation and relieve pain. Be sure to follow the recommended dosage and consult a doctor if needed.
Stretching exercises
Stretching your calf muscles, Achilles tendon, and the plantar fascia can help alleviate your pain and prevent stiffness. Simple exercises like towel stretches or calf stretches can improve your flexibility and reduce the strain on your foot.
Foot supports
Wearing supportive shoes with proper arch support and cushioning can reduce pressure on your plantar fascia. Orthotic insoles may also help distribute pressure more evenly across your foot.
Night splints
Wearing night splints can help maintain a light stretch of the plantar fascia while you sleep. This helps prevent the fascia from tightening during the night and reduces morning pain.
How to Prevent Plantar Fasciitis
Preventing plantar fasciitis is possible but it involves making adjustments to your daily habits and lifestyle.
How to prevent plantar fasciitis:
Wear proper footwear – Select footwear that provides the right arch support, cushioning, and stability for your heels. Avoid walking barefoot on hard surfaces and limit prolonged use of high heels to reduce strain on your feet.
Regular Stretching – Regularly stretch your calves, Achilles tendons, and feet to improve flexibility and reduce the risk of strain on the plantar fascia.
Maintain a healthy weight – Keeping your weight within a healthy range will help to reduce the strain on your feet, decreasing your chances of developing plantar fasciitis.
Take breaksto rest – If you stand or walk for long periods, take breaks to rest your feet and alleviate pressure. If you can't take breaks, alternating between sitting and standing can also help prevent overuse.
Strengthen your feet and lower legs – Exercises that strengthen your calf muscles, foot muscles, and ankle stabilizers can help prevent plantar fasciitis by improving foot mechanics and reducing excessive strain.
Exercises to Help Release and Heal Plantar Fasciitis
Here are some targeted exercises to help with plantar fasciitis:
Towel Stretch – Sitting on the floor with your legs stretched out in front of you, wrap a towel around the ball of your foot. Gently pull your foot toward you, feeling a stretch along the bottom of your foot and the back of your leg.
Calf Stretch – Stand arm's length facing a wall and step back with one leg. Keep your back leg straight and your heel planted on the ground. Place your hands on the wall at the height of your shoulders and lean forward, stretching your calf and Achilles tendon of your back leg.
Foot Roll – To help massage the plantar fascia and relieve built-up tension, you can use a tennis ball or similar ball under the arch of your foot. Once you place it, slowly roll it back and forth.
Toe Stretch – While sitting with your legs extended, reach for your toes and gently pull them toward your body. This stretch helps loosen the plantar fascia and should be held for 15-30 seconds before repeating.
Heel Raises – Stand with the balls of your feet on the edge of a step. Slowly lift yourself onto your toes, then lower your heels past the level of the step to stretch your calves and the bottom of your feet.
Whether you're a runner, a retail worker, or someone who loves their flip-flops a little too much, plantar fasciitis can sneak up on you. Knowing your risk factors is half the battle. With the right footwear, regular stretching, and paying attention to heel pain symptoms, you can take steps (literally!) to protect your feet.
Plantar fasciitis doesn't have to be a permanent issue. You can effectively manage and treat this painful condition with proper care, early intervention, and lifestyle adjustments. If your at-home treatments aren't bringing you relief or if your symptoms are worsening, Princeton Orthopaedic Associates is here to help. Our team of specialists can provide targeted therapies, advanced treatments, and personalized care to help you get back on your feet and live pain-free.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
Could Your Neck Pain Be a Pinched Nerve in the Neck?
You wake up with a stiff neck, thinking you just slept in an odd position. But as the day goes on, the pain doesn't go away. Instead, it radiates down your shoulder and into your arm. Simple tasks like turning your head, reaching for your phone, or even sitting at your desk become uncomfortable. You think, maybe you just slept weird and it will feel better tomorrow, except the pain doesn't improve, it continues for days, even weeks. This is what living with a pinched nerve in the neck can feel like—persistent discomfort that affects your daily life.
What is a Pinched Nerve in the Neck?
A pinched nerve in the neck, also known as cervical radiculopathy, occurs when excessive pressure is applied to a nerve root in the cervical spine (neck area). This pressure can come from surrounding structures such as bones, cartilage, muscles, tendons, or swollen tissues, leading to nerve irritation or compression. This compression disrupts the nerve's normal function and can lead to pain, tingling, weakness, or numbness in your neck.
Symptoms of a Pinched Nerve in the Neck
The symptoms you experience from a pinched nerve in the neck can vary from person to person, but generally speaking, the most common symptoms often involve a discomfort that radiates beyond your neck. You may experience a sharp or burning pain that extends into the shoulder, arm, or even down to the fingers, sometimes worsening with certain movements or prolonged positions. With the pain, there may be an unusual tingling or buzzing sensation, almost like the affected area has "fallen asleep," which can become persistent or intermittent. You may also notice weakness in their grip or find it harder to perform tasks requiring fine motor skills, as the nerve's ability to send signals to the muscles is compromised. In more severe cases, prolonged compression can lead to a feeling of numbness or loss of sensation in certain areas, making it difficult to tell if you're touching something or feeling temperature changes properly.
Symptoms of a pinched nerve in the neck:
Pain in your neck: Sharp, aching, or burning pain localized in the neck area.
Radiating pain or discomfort extending from your neck to your shoulder, arm, or even fingers.
Limited range of motion – Difficulty turning your head or tilting your neck without pain.
Numbness or tingling: A sensation of reduced or lost feeling in the affected area, sometimes accompanied by a "pins and needles" or prickling feeling.
Muscle weakness – Difficulty lifting objects or performing everyday tasks due to weakened muscles.
Why you can trust us:
We have multiple highly specialized, board-certified, fellowship-trained orthopaedic surgeons.
We know that we serve people - actual humans - not random orthopaedic conditions. That drives us to compassionate care.
The world of orthpaedics is constantly evolving. Our orthopaedic surgeons are constantly evaluating new techniques, tools and methods to serve our community even better.
We provide outcome-focused treatment. We work with our patients to achieve their goals, all while developing custom treatment plans that fit our patient's lives.
The causes of a pinched nerve in the neck can vary from person to person, but generally speaking, they stem from excessive pressure or irritation affecting the nerves in your spine in the neck. In many cases, age-related changes in the spine, such as degenerating discs or bone spurs, gradually narrow the space where nerves exit, leading to compression. Injuries, like sudden whiplash from a car accident or repetitive strain from poor posture, can also cause misalignments or inflammation that presses on the nerve. For some people, long hours spent looking down at a phone or sitting at a desk with improper ergonomics contribute to chronic strain, gradually leading to nerve irritation. Inflammatory conditions, like arthritis, or acute issues, such as a herniated disc leaking fluid onto nearby nerves, can also increase pressure, intensifying symptoms over time.
Causes of a pinched nerve in the neck:
Poor posture – Slouching or looking down at screens for long periods strains your neck.
Herniated disc – When the soft inner material of a spinal disc pushes through its outer layer. When doing so, it can create pressure on nearby nerves, leading to pain and discomfort.
Bone spurs – Overgrowth of bone in your spine can narrow the spaces where nerves travel.
Arthritis – Inflammation and degeneration of joints can lead to nerve compression.
Injury – Sudden impacts from accidents or sports can lead to nerve irritation.
Repetitive motions – Constant strain from work or activities like texting or carrying heavy bags can contribute.
When to Seek Care from an Orthopedic Spine Specialist
Pain persists for several weeks despite home treatments.
Weakness in your arms or hands affects daily tasks.
Loss of coordination or balance signals nerve damage beyond just discomfort.
Symptoms worsen over time, even with rest and self-care.
Loss of bowel or bladder control can sometimes happen and may indicate a more serious spinal condition requiring immediate attention.
How to Treat a Pinched Nerve in the Neck at Home
A pinched nerve can cause discomfort ranging from mild tingling to sharp, radiating pain that disrupts daily life. Whether it’s in your neck, back, or another area, this condition occurs when surrounding tissues—such as muscles, tendons, or bones—put excess pressure on a nerve. While severe cases may require medical attention, many pinched nerves can be relieved at home with simple, effective treatments.
From gentle stretches and posture adjustments to anti-inflammatory remedies and nerve-soothing techniques, here’s how you can ease pain and support your body’s natural healing process:
Rest and avoid aggravating movements – Rest is always important when it comes to home treatment. Try to minimize activities that strain your neck. Continued stress can worsen your inflammation and lengthen the time it takes for you to heal. Resting allows the affected nerve to recover without further irritation.
Apply heat or ice – Applying an ice pack to your neck within the first 48 hours of injury can help reduce swelling and numb pain. After the initial inflammation subsides, switching to a heating pad or warm compress can help improve blood circulation and relax tense muscles around the nerve.
Use over-the-counter pain relievers – Medications such as ibuprofen or naproxen can help alleviate pain and reduce inflammation, making it easier to perform daily tasks while healing.
Adjust your sleeping position – Sleeping with a supportive pillow, one that keeps your neck aligned with your spine, can relieve pressure on your pinched nerve. Sleeping on your back or side rather than your stomach is also beneficial to avoid excessive neck strain.
Gentle stretching – Performing slow and controlled neck stretches can help release the pinched nerve and improve mobility. Simple exercises such as chin tucks, neck tilts, and shoulder rolls can gradually reduce tension and enhance flexibility.
Maintain good posture – Practicing proper posture while sitting, standing, and using electronic devices can prevent further nerve compression. Keeping your shoulders back and your head aligned with your spine can significantly reduce neck strain.
Massage therapy – Massaging your neck and shoulder muscles can help improve circulation, reduce muscle tension, and promote relaxation.
Meet Our Orthopaedic Spine Specialists
How to Prevent a Pinched Nerve in the Neck
Preventing a pinched nerve in the neck starts with maintaining good posture, keeping muscles strong and flexible, and avoiding repetitive strain. Poor posture, prolonged screen time, and sleeping in awkward positions can all contribute to nerve compression, leading to pain, stiffness, and discomfort. By making small adjustments—such as improving ergonomics, incorporating regular stretching, and strengthening the neck and shoulders—you can reduce the risk of nerve irritation and keep your neck healthy and pain-free.
Here’s how to take proactive steps to prevent a pinched nerve before it starts.
Practice good posture – Keeping your head aligned with your spine reduces unnecessary strain on your neck. When working at a desk, ensure your monitor is at eye level, and your shoulders remain relaxed.
Take breaks from screens – Looking down at your phone or computer screen for long periods stresses your cervical spine. Taking frequent breaks, using a stand for devices, and adjusting screen height can help minimize the risk of nerve compression.
Strengthen your neck and shoulder muscles – Strengthening exercises such as chin tucks, shoulder blade squeezes, and resistance training can provide better support for your neck, reducing the likelihood of nerves becoming pinched.
Use proper ergonomics – Adjusting your workstation to include a supportive chair, a desk at the correct height, and a keyboard to encourage natural wrist alignment can prevent awkward neck positions contributing to nerve compression.
Avoid carrying heavy bags on one side – Carrying a heavy purse, backpack, or briefcase on one shoulder creates an imbalance that strains your neck muscles. Opt for a backpack with even weight distribution or frequently switch sides to help reduce stress on your cervical spine.
Sleep with proper support – Choosing a pillow that maintains the natural alignment of your neck and adopting a sleep position that keeps your spine in a neutral posture can help reduce strain and prevent excessive pressure on cervical nerves.
Maintain an active lifestyle – Regular exercise promotes flexibility, strengthens muscles, and improves overall spinal health, reducing the risk of nerve compression over time.
Exercises to Help Release and Heal a Pinched Nerve
When dealing with a pinched nerve, gentle movement and stretching can help alleviate pressure, improve mobility, and promote healing.
Below is a more detailed explanation of how to perform each exercise effectively:
1. Chin Tucks
Purpose: Strengthens the deep neck flexors, improves posture, and reduces strain on the cervical spine.
How to Do It:
Sit or stand with your spine straight.
Gently pull your chin straight back (as if making a double chin), keeping your head level.
Hold for 5-10 seconds, then relax.
Repeat 8-10 times.
Tip: Avoid tilting your head up or down—think of sliding your head straight back.
2. Neck Side Bends (Lateral Flexion Stretch)
Purpose: Stretches the muscles along the sides of your neck to reduce tension.
How to Do It:
Sit or stand with your shoulders relaxed.
Slowly tilt your head to one side, bringing your ear toward your shoulder.
Hold for 15-30 seconds, feeling the stretch along the opposite side of your neck.
Switch sides and repeat 3-5 times per side.
Tip: Keep your shoulders down and relaxed to get the full benefit of the stretch.
3. Neck Rotations
Purpose: Increases flexibility and reduces stiffness in the neck.
How to Do It:
Sit or stand with a straight back.
Slowly turn your head to the right, trying to look over your shoulder.
Hold for 5-10 seconds, then return to the center.
Repeat on the left side.
Do this 5-8 times on each side.
Tip: Move slowly and avoid forcing the stretch. If you feel pain, stop immediately.
4. Shoulder Rolls
Purpose: Relieves tension in the shoulders and neck, improving blood flow.
How to Do It:
Sit or stand with your arms relaxed at your sides.
Roll your shoulders forward in a circular motion 10 times.
Reverse the motion and roll them backward 10 times.
Tip: Perform this exercise slowly and deliberately, focusing on releasing tension in your upper back and neck.
5. Upper Trapezius Stretch
Purpose: Helps release tightness in the upper shoulders and neck, which can contribute to nerve compression.
How to Do It:
Sit or stand with a straight posture.
Tilt your head toward one shoulder.
Use your hand on the same side to apply light pressure, gently deepening the stretch.
Hold for 15-30 seconds, then switch sides.
Repeat 3-5 times per side.
Tip: Keep your opposite shoulder relaxed and down to maximize the stretch.
Final Tips:
Perform these exercises gently—never force a stretch.
Consistency is key; do them daily for best results.
If you experience sharp pain or worsening symptoms, stop immediately and consult a healthcare provider.
A pinched nerve in your neck can make daily activities difficult, but you don't have to live with chronic pain. You can find relief and restore normal function with proper care, treatment, and lifestyle adjustments. Our spine specialists here at Princeton Orthopaedics Associates are here to help if your symptoms persist or worsen. Reach out today for expert care and personalized treatment options to get you back to living pain-free.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.
Peroneal Tendonitis
Peroneal tendonitis is a common yet also misunderstood condition affecting the outer portion of your ankle; it can cause you significant discomfort and interfere with your daily activities if left untreated. This condition often arises due to overuse, sudden changes in physical activity, or biomechanical issues that strain the peroneal tendons. While athletes and active individuals are particularly susceptible, anyone can develop peroneal tendonitis if the tendons are subjected to excessive stress. Understanding the anatomy, causes, symptoms, and appropriate care is crucial for effective management and prevention.
Understanding peroneal tendonitis, its anatomy, common causes, symptoms, treatment options, and how to prevent it can help you recover and get out of pain!
What Is Peroneal Tendonitis?
Peroneal tendonitis, also known as peroneal tendinopathy, can also be referred to by other names, including:
Peroneal tendonitis is the most commonly used term.
Peroneal tendinopathy is a medical term that describes any damage or disorder of the tendon without specifying inflammation.
Peroneal tendon inflammation is a more specific name indicating the inflammation of the peroneal tendons.
Peroneal tenosynovitis refers to inflammation of the synovial lining around the tendon, though this is a less common term.
Peroneal tendonitis refers to irritation or inflammation of the peroneal tendons, which run along the outer side of your ankle. These tendons are important for stabilizing your ankle joint and facilitating foot movement. When these tendons become inflamed, they can cause pain, swelling, and reduced mobility. This condition is most frequently seen in individuals who engage in repetitive ankle movements, but it can also arise from acute injuries or biomechanical abnormalities.
Specifically, there are two peroneal tendons involved in peroneal tendonitis:
Peroneus Longus: This tendon runs behind the bony prominence on the outer ankle (the lateral malleolus ) and extends underneath the foot to the arch. It helps turn the sole of the foot outward (foot eversion) and supports the foot's arch.
Peroneus Brevis: This tendon also runs behind the lateral malleolus but attaches to long bone of the outer edge of the foot. It assists with ankle stability and eversion.
Peroneal tendonitis typically develops due to overuse, resulting in micro-tears and inflammation within the tendons. This condition can occur in one ankle (unilateral) or, less commonly, in both ankles (bilateral).
Causes of Peroneal Tendonitis
Peroneal tendonitis can result from various causes, often related to repetitive motion or biomechanical stress. Identifying and addressing these underlying causes is key to both treatment and prevention.
Overuse or Repetitive Motion:
Athletes who engage in activities involving repetitive ankle movement (e.g., running, hiking, or sports requiring quick lateral motions) are at greater risk. Over time, repetitive stress can lead to micro-tears in the tendons, causing inflammation and pain.
Sudden Increase in Physical Activity:
If you have a rapid increase in exercise intensity or frequency, it can strain your peroneal tendons. For instance, starting a new running regimen or abruptly increasing training volume can place excessive stress on the tendons.
Wearing Improper Footwear:
If you wear shoes that lack proper support, they can increase stress on the peroneal tendons. Poor arch support or insufficient cushioning can alter your foot mechanics and contribute to the irritation of your tendons.
Foot and Ankle Misalignment:
High arches or an abnormal gait can increase tendon strain. Individuals with these anatomical variations are more prone to overloading the peroneal tendons.
Previous Ankle Injuries:
A past ankle injury, like an ankle sprain, can increase your risk of developing peroneal tendonitis. If you have a history of ankle sprains or instability, you can be more susceptible because these injuries can weaken the tendons, making them more prone to inflammation.
Ankle instability:
Weakness or poor coordination in the ankle can contribute to stress on the tendons.
Biomechanical issues:
Abnormalities in the way the foot moves (like flat feet or high arches) can lead to additional stress on the tendons.
Underlying conditions, such as inflammatory arthritis or connective tissue disorders, can also weaken the tendons or increase inflammation, predisposing people to peroneal tendonitis.
Symptoms of Peroneal Tendonitis
These are the common symptoms of peroneal tendonitis:
Experiencing pain along the outer side of your ankle: This pain is usually located behind the bump on the outside of your ankle, the lateral malleolus, and may worsen with movement.
Ankle Swelling and tenderness: The affected area of your ankle may become swollen, and the tendons themselves may also be tender to the touch.
Ankle pain that worsens with physical activity and improves with rest: Activities such as walking, running, or standing for long periods typically aggravate symptoms, but they reduce after rest and avoiding said activities.
A sensation of ankle instability or a snapping feeling: In some cases, the tendons may slip out of their normal position, causing a noticeable snapping sensation.
Stiffness or weakness: Individuals may experience stiffness when moving the ankle, as well as weakness during activities requiring ankle stability.
Home Care for Peroneal Tendonitis
If you suspect you have peroneal tendonitis, early intervention with home care is essential for symptom management and recovery. Consistent and proactive home care can prevent the condition from worsening and promote healing. Consider the following steps:
Rest: Avoid activities that exacerbate pain to allow the tendons to heal. Continuing strenuous physical activity can worsen inflammation and prolong recovery time.
Ice Therapy: Apply ice to the outside ankle area for 15-20 minutes. Do this every 2-3 hours to help reduce inflammation. Be sure to use a cloth between the ice and your skin to protect your skin and prevent frostbite.
Ankle Compression: Use an elastic bandage or ankle brace to provide support and minimize swelling. This can also offer additional stability to a weakened ankle.
Elevation: Keep the ankle elevated above heart level when resting to decrease swelling. Elevating the affected limb can reduce fluid buildup and ease discomfort.
Anti-Inflammatory Medications: Over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen can help relieve pain and inflammation. Follow dosage guidelines carefully and consult a healthcare provider if you have any concerns.
Why you can trust us:
We have multiple highly specialized, board-certified, fellowship-trained orthopaedic surgeons.
We know that we serve people - actual humans - not random orthopaedic conditions. That drives us to compassionate care.
The world of orthpaedics is constantly evolving. Our orthopaedic surgeons are constantly evaluating new techniques, tools and methods to serve our community even better.
We provide outcome-focused treatment. We work with our patients to achieve their goals, all while developing custom treatment plans that fit our patient's lives.
While mild cases of peroneal tendonitis may resolve with home care, we recommend you seek medical attention right away if you experience:
Persistent pain despite rest and self-care: If symptoms do not improve within a few weeks, a comprehensive medical evaluation may be necessary.
Significant swelling or bruising: Extensive swelling or discoloration around the outside of your ankle could indicate more severe tendon damage or an associated injury.
Ankle instability or difficulty bearing weight: Persistent instability or an inability to walk comfortably warrants a specialist's assessment.
Popping or snapping during movement: If you feel a popping or snapping sensationd uring movment, this may suggest tendon subluxation (displacement) or a partial tear which would require professional intervention.
Treatment depends on the severity of the condition and may include:
Physical Therapy: Customized exercise programs can restore strength and improve range of motion. Therapists may also use techniques like ultrasound therapy to help promote your healing.
Immobilization: Severe cases may require a walking boot or brace to limit motion and promote healing. Immobilization prevents further strain and allows the tendons to repair themselves.
Orthotics: Custom insoles can correct biomechanical issues and relieve tendon stress. Proper foot alignment reduces the likelihood of recurrence.
Steroid Injections: In some cases, corticosteroid injections may be discussed and can reduce persistent inflammation. Use of these injections will be determined by you and your treating physician.
Surgery: Rarely, surgery is required to repair tendon tears or address chronic instability. Surgical intervention may involve tendon repair, cleaning inflamed tissue, or stabilizing the tendons.
Preventing Peroneal Tendonitis
Proactive measures can reduce the risk of developing peroneal tendonitis, especially for those prone to ankle injuries. Consider incorporating the following strategies:
Strengthening Exercisesfor Peroneal Tendonitis: Targeting the ankle and foot muscles enhances stability and reduces strain. Examples include:
Ankle Eversion Exercise: Use a resistance band to strengthen the peroneal muscles. This improves tendon resilience and stability.
Calf Raises: Improve overall ankle strength by lifting onto your toes and slowly lowering down. Perform both double-leg and single-leg variations for comprehensive strengthening.
Balance Exercises: Perform single-leg stands to enhance proprioception and stability. Balance drills can help prevent future injuries by improving coordination.
Supportive Footwear: Choose shoes with enough arch support and cushioning, especially for high-impact activities. Custom orthotics may also be beneficial if you have high arches or foot misalignment.
Gradual Progression: Increase physical activity levels gradually to prevent overuse. Sudden increases in intensity or duration should be avoided.
Stretching Routine: Regularly stretch the calf muscles and ankles to maintain flexibility. Flexible tissues are less prone to injury and inflammation.
If you're experiencing persistent ankle pain or instability, it's essential to seek professional care. The specialists at Princeton Orthopaedic Associates are here to provide expert diagnosis and personalized treatment plans. Schedule a consultation today to get back to the activities you love with confidence.
If you're experiencing hand cramps, or muscle cramps in your hands, it can significantly affect your daily activities. Whether you're typing on a keyboard, cooking a meal, or simply opening a bag or a jar, hand cramps can make these simple, everyday tasks frustrating and sometimes painful. For some people, hand cramps may start subtly—a slight stiffness or discomfort that comes and goes. Over time, the cramps may become more intense and frequent, interfering with work, hobbies, and everyday routines.
Hand cramps are a common yet bothersome issue that can affect anyone. These sudden, involuntary muscle contractions in the hands can cause discomfort, disrupt daily routines, and strike at the most inconvenient times. Understanding why you're experiencing hand cramps is the first step toward finding relief and preventing future episodes.
What Are Muscle Cramps in Hands?
Hand cramps are involuntary muscle spasms or contractions in your hands and fingers. They can appear gradually and range from mild twitching to intense pain and stiffness. Initially, you may notice a mild tightening or twitching sensation in your fingers or palm. As the cramps progress, the stiffness can become more pronounced, sometimes accompanied by sharp or throbbing pain. You might experience involuntary muscle spasms, making it difficult to control fine motor movements.
They can last a few seconds or persist for several minutes and worsen without intervention, making it difficult to use your hands comfortably. Occasional hand cramps may be harmless, but persistent or severe cramping could indicate an underlying health issue that needs attention.
Symptoms of Hand Cramps
It can be easy to ignore or push away the issues you are having with hand cramps, but recognizing the symptoms of when hand cramps are an issue can help you identify and manage them effectively.
While the individual intensity and duration of cramps can vary, the following symptoms are common:
Sudden Muscle Contractions:
Experiencing sudden, involuntary tightening or spasms in the hand muscles that occur unexpectedly and range from mild to severe.
Tingling or Numbness:
Experiencing a prickling sensation or temporary loss of feeling, often caused by poor circulation or nerve compression, may accompany you hand cramps.
Stiffness:
Reduced flexibility in the hands and fingers can make movement difficult and impede the completion of daily tasks.
Pain and Discomfort:
It's common to experience mild to severe aching or sharp pain accompanying muscle cramps; this pain may also linger after the cramp subsides.
Tightness or Swelling:
Experiencing a sensation of fullness or visible swelling in the affected area can indicate muscle strain or fluid retention, further contributing to discomfort.
Fingers Curling or Locking:
Temporary and involuntary bending of the fingers, causing temporary stiffness or difficulty straightening them.
Difficulty Gripping Objects:
Struggling to hold or carry items due to hand stiffness, weakness, or sudden cramps.
Why you can trust us:
We have multiple highly specialized, board-certified, fellowship-trained orthopaedic surgeons.
We know that we serve people - actual humans - not random orthopaedic conditions. That drives us to compassionate care.
The world of orthpaedics is constantly evolving. Our orthopaedic surgeons are constantly evaluating new techniques, tools and methods to serve our community even better.
We provide outcome-focused treatment. We work with our patients to achieve their goals, all while developing custom treatment plans that fit our patient's lives.
Certain daily activities can increase the likelihood of experiencing hand cramps due to muscle strain or fatigue. Identifying your specific triggers can help you make changes to reduce the frequency and intensity that you experience issues with your hands cramping.
Common daily-life causes of muscle cramps in your hands:
Frequent Typing and Desk Work: Extended periods of typing or using a mouse can strain hand muscles. Poor ergonomics and repetitive movements increase the risk of muscle fatigue, leading to cramps. If you spend hours working on a computer without adequate breaks, your hand muscles may become overworked and become prone to spasms.
Lifting Heavy Objects: Frequent lifting or gripping heavy items can overwork the hand muscles, causing painful cramps and muscle tightness. This is particularly common in professions requiring manual labor or during intensive household tasks.
Waking Up From Sleep: Sleep positions that restrict blood flow or place pressure on the hands can lead to morning hand cramps. You may experience a tight, clenched sensation upon waking up, especially if your hands were in an awkward position during the night.
Cooking and Food Preparation: Repetitive hand motions like chopping, cutting, and stirring can cause muscle strain, resulting in sudden cramping sensations. Prolonged food preparation sessions without breaks can exacerbate the issue.
Sports and Physical Activity: Activities that require repeated or forceful hand movements, such as tennis, golf, or weightlifting, can cause cramping due to muscle overuse. Athletes and fitness enthusiasts who push their muscles without sufficient recovery time are particularly vulnerable.
Physical and medical causes of muscle cramps in your hands:
Several physical factors can contribute to hand cramps. Identifying the underlying cause is crucial for effective treatment and prevention.
Here are the most common causes:
Muscle Overuse and Fatigue: Repetitive hand movements without adequate rest can fatigue the muscles, causing cramps. This is common in individuals who type extensively, play musical instruments, or perform manual labor. Overuse can lead to muscle strain, which increases the likelihood of involuntary contractions.
Dehydration: Insufficient hydration can disrupt the balance of electrolytes like potassium and magnesium, leading to muscle cramps. Muscles rely on proper fluid levels to contract and relax efficiently, so staying well-hydrated is essential to maintain optimal muscle function.
Poor Circulation: Conditions that impair blood flow, such as Raynaud's disease or carpal tunnel syndrome, can cause hand cramps by limiting oxygen delivery to muscles. Restricted circulation reduces the availability of essential nutrients, increasing the risk of cramping.
Nutrient Deficiencies: A lack of essential minerals, particularly magnesium, potassium, and calcium, can increase the likelihood of muscle cramps. These nutrients play a vital role in muscle contraction and nerve function, and a deficiency may lead to frequent spasms.
Underlying Medical Conditions: Chronic health issues like arthritis, diabetes, and thyroid dysfunction can affect nerve and muscle health, leading to frequent hand cramps. Neuromuscular conditions can interfere with the normal function of your muscles and cause persistent cramping.
What to do For Muscle Cramps in Hands
If you want to get rid of muscle cramps in your hands, several strategies can provide immediate relief and help prevent future occurrences. Implementing these techniques can reduce the severity and frequency of cramps:
Stretching and Gentle Exercise: Perform regular hand and finger stretches to maintain flexibility and reduce muscle tension. Gentle stretching increases blood flow, helps muscles relax, and alleviates cramps while preventing future occurrences.
Stay Hydrated: Ensure you drink plenty of water throughout the day to prevent dehydration and maintain proper electrolyte balance. Hydrated muscles are less likely to cramp, especially during periods of physical activity.
Warm Compress: Applying a warm compress or soaking your hands in warm water can soothe cramped muscles and enhance blood flow, relieving stiffness and discomfort. Heat therapy can be particularly effective when cramps are caused by poor circulation or muscle fatigue.
Massage Therapy: Gently massaging the cramped muscles improves circulation and promotes muscle relaxation. Apply light pressure to the affected area using your opposite hand to ease tension and encourage blood flow.
Ergonomic Adjustments: Optimize your workstation with ergonomic tools to reduce strain on your hands. Use a comfortable chair, position your keyboard properly, and take regular breaks to stretch. These adjustments can prevent repetitive strain and muscle fatigue.
Dietary Supplements: If you have a confirmed nutrient deficiency, consider taking magnesium or potassium supplements after consulting with a healthcare professional. These minerals play a crucial role in muscle relaxation and nerve signaling, which can prevent future cramps.
While occasional hand cramps are usually harmless, persistent or severe cramps may indicate an underlying medical condition. You should consult an orthopaedic hand specialist if you experience:
Frequent or worsening hand cramps.
Persistent numbness or tingling.
Hand weakness or loss of function.
Cramping that interferes with daily activities.
Our hand specialists can diagnose the cause of your hand cramps and recommend appropriate treatments, such as physical therapy, medication, or specialized care.
Prevention: How to Stop Muscle Cramps in Hands
If you are prone to experiencing hand cramps, you can reduce the frequency and intensity of hand cramps by taking proactive measures.
Similar to treatment for hand cramps but not quite the same, here are some prevention tips:
Hydrate Adequately: Drink sufficient water daily to maintain muscle function and prevent cramps.
Maintain Balanced Nutrition: Ensure your diet includes essential minerals like magnesium, potassium, and calcium.
Practice Regular Stretching: Incorporate hand and finger stretches into your routine to maintain muscle flexibility.
Use Ergonomic Tools: Adjust your work environment to minimize hand strain and fatigue.
Take Breaks: Allow your hands to rest during repetitive tasks to prevent overuse and muscle exhaustion.
Experiencing hand cramps can be uncomfortable and disruptive to your daily functioning. Understanding their causes and adopting preventive measures can help you manage and reduce their occurrence. However, if you are dealing with persistent symptoms, seeking medical advice is essential to identify and address any underlying health conditions and set you down the right treatment path.
This blog post is meant to be informative and should not act as a self-diagnosis tool. If you’d like to see one of our doctors, please contact us here.